I used to have angina before. Now, I am fine doctor but confused after undergoing this angiogram. I need an opinion.
How is your exercise capacity?
I do walk, work, and able to do almost all regular activities.
Why did you do this angiogram then?
Had to undergo this after a doubtful stress test, Now, I am told by at least 2 eminent cardiologists, that I am having just one functional coronary artery, and it is dangerous for the all-important LAD to live at the mercy of RCA. They said they will try to fix it with wires first or CABG if it failed.
After explaining the excellent backup from RCA to LAD, I told him, “Yes, most scientific cardiologists are not trained to respect collateral circulations, in spite of the fact, many CTOs fall under class 3 (contra)Indication for revascularisation. I must admit I am not that scientific but it ensures my patients don’t really suffer unnecessarily”
“Make a pardon doctor, I didn’t get you, what I am supposed to do ?”
I meant, your collateral circulation is good enough and you may not need any intervention.
Are you sure doctor?
I don’t know why I was so blunt in my response“If you believe me forget the lesion. If you don’t, get it stented or go for CABG as per the majority advice of the eminent “. I am sorry. I think I cleared your confusion.
Coronary collateral circulation is one of the major determinants of symptoms and outcomes in chronic CAD. But, we generally shrug off the value of coronary collateral circulation in acute coronary syndrome. The fact is, it has a myocardial mitigating effect following sudden total occlusion.
When does it appear? We did a small analysis (PDF version)
We found it is noted in 25% of patients. With reference time of appearance, 6% had it within 12hrs and in few, it was noted as early as 6 hrs. One caveat is, we may not know whether its preexisting collateral due to chronic multivessel CAD. I am sorry to note this study did not address the outcome analysis. We however documented patients with good collaterals had negligible wall motion defect and near-normal function post PCI. Some of you can pursue research in this area.
Potential role of collaterals in ACS
It limits the infarct size
Keep the myocardium alive and give us time to intervene
Can converts a potential Q-MI to non-Q MI
Possibly prevent primary VT/VF and hence dreaded sudden death in early STEMI
Prevent early adverse remodeling of the left ventricle.
When these points appeared just my assumptions, Dr. Ali Aldujeli, (Lithuanian University of Health Sciences, Kaunas) in his presentation, at TCT 2020 confirms many of them are Indeed true
Final message
I agree, in the era of instant gratification with primary PCI, relying on coronary collaterals may appear a lesser professional virtue. Still, we may need to respect nature. Many times it bails us out.
Note :This is a copy of my earlier blog on coronary micro-circulation published few years ago.Recently this got numerous hits .Hence I have just reposted it with slight modification.
Human coronary circulation stands unique among others as it is a life-sustaining circulation.It is indeed a great medical achievement to visualise the right and left coronary artery system by coronary angiogram. Actually, what we see is only a fraction of the surface area of coronary circulation .The surface area of epicardial coronary arteries constitutes less than 5 % of entire coronary vascular tree .
This is the reason normal coronary angiogram can never mean normal coronary circulation !
This huge gap in our perception is the single important factor that explains the vagaries of modern coronary care .
This also make any clinical coronary scenario a reality .
“A patient with normal coronary angiogram getting a myocardial infarction , the next day and a severe triple vessel disease living comfortably for decades with medical management”
So , it is essentially a false sense of scientific accomplishment by the cardiac scientists at least in the of coronary circulatory physiology.
What determines the extent of these invisible coronary micro circulation ?
There are innumerable channels of micro vessels traversing across the heart, sharing , bridging , branching, penetrating and perfusing the muscle mass.They can be anatomically patent , physiologically non patent .They can be recruited by hemodynamic stress .These are never visualized by current imaging modalities..It is also influenzed by favorable growth milieu and hormonal and neural stimuli.
Ignorance based cardiology
What is the mechanism of primary VF following acute STEMI ?
The quantum of coronary micro circulation is like the vast cerebral neuronal net work .We have every reasons to believe they are have unique genetic imprint.How else you can explain a man with full blown STEMI come 24 hours later comfortably to the OPD while another loses his life with a stormy primary VF before even boarding the ambulance !
Why many cardiologists do not give due credit the coronary collateral circulation ?
It has been our traditional teaching ( without much evidence of course !) coronary collateral circulation is not effective to support blood flow during exercise . This fact has been disproved many times . Coronary collateral circulation was indeed useful in limiting damage in ACS and relieve symptoms in stable angina.It helps in reverse remodeling and provided electrical stabilty as well in post MI population.
Still , the concept was alienated and made totally irrelevant in the interventional era . Many cardiologists found well-developed collateral’s as an interference to their expertise and ego since it has a potential to alter the indication of PCI.They continue to have strong scientific conviction (Pseudo ?) that man made collaterals must always been superior to God made collaterals !
Whenever some credible reports emerge about collateral circulation being equivalent to revascularisation procedure , these concepts were prematurely buried for some reason.
In the last decade there was a concern about performing PCI in patients with well-developed collaterals .The argument was , they tend to develop early stent occlusion and restenosis . It was a genuine query raised by few thought leaders in the field as collateralised vessels suffer from low flow after PCI , if the pre -existing collateral continue to function.
But then , few studies countered this , and PCI was shown to be safe and in fact may fare well in patients with extensive collaterals .
In these studies interventionist’s argument looked amusing ! as they seem to define a successful PCI as not only to open the occluded vessel but also make sure to close all functioning collaterals .(What a a pity for our natural biological angiogenic forces which had worked and grown meticulously for months!)
Cardiac science in the current format, makes the future look bleak for coronary a collateral circulation .With early PCI becoming a norm we will never ever allow the natural collaterals to grow , and even the established collaterals will have to face a stiff fight for survival with sophisticated coronary interventions .
Competing interest in the filed of coronary collateral research
While the basic scientists want to grow collaterals with angiogenesis , stem cells etc interventionists continue to indulge in rampant angioplasties which will suppress collateral growth.
This implies we will struggle to establish the true importance of coronary collateral circulation .
Final message
Can it be an effective form of revascularisation ?
My personal inference is coronary collateral circulation “would and should” have a definite role in at- least some of the subsets with chronic coronary syndromes. If we think otherwise . . . it’s against the principle of natural biological science .
A good collateral system with optimal medical management can save not only our patient’s lives but also their hard earned currencies !
Reference
Here is a rare article in European heart journal that discuses coronary collateral circulation . Let us welcome such wonderful reviews which keep the interest alive on the filed.
I get frequent comments about my blog. I do try to answer many of them . This is a very unique one , and it is making me think further.Since he has specifically wished his clinical data could be eye opener for others , I am jut posting it here . The comment was in response to my article Who said coronary collateral circulation will not support exercise ? here is the extract
Dr. Venkatesan,
I read your blog with great interest and I think I may have something useful to contribute from my own personal experience. I am a 68 year old male with a long history of smoking (for fifty years), and a history of uncorrected hypertension over the years (it has been corrected to normal with medication for many years now). I am a non-smoker now for the past 18 months. I have PAD and a moderate aortic aneurysm of about 3.5CM (ascending and descending) which is being watched with regular vascular scans.
The common femoral arteries in both of my legs are nearly 100% occluded between my thighs and my knees, and yet my ankle and toe blood pressures (and my circulation in my ankles and feet) is almost normal. The reason for that is that according to the vascular scan, my deep femoral arteries are much larger caliber than normal with extensive vascular collateralization by passing the common femoral occlusions.
About twenty years ago before the PAD diagnosis, I realized that I had claudication in both of my calves when I walked a short distance. I expected this was being caused by an arterial blockage in my legs, so I went to the gym every day for about three years, and walked through the pain every day. I believe this contributed to the formation of the collaterals that have perhaps saved my legs and feet.
I also have heart disease, and had a fairly minor heart attack in 1999. No stents were placed nor angioplasty performed at that time. I recently had an arteriogram and cardiac stress MRI which showed that two of the three coronary arteries are now 100% occluded (apparently I had another cardiac event and did not know it). The cardiologist says that the LAD is in extremely good condition and has numerous collaterals branching from it. I have no symptoms whatever from all of this, except that my LVEF is low (about 35%). I walk at a very brisk pace six miles per day, five days per week, and I monitor my pulse rate with a pulse monitor when I walk. I keep my pulse between 115 and 120 which I calculate to be 80% of maximum for my age. I believe this cardio exercise / walking has also helped with the collateral formation, and I am hoping to bring the LVEF back up to a reasonable number with this exercise regimen.
My cardiologist has recommended an ICD, but I have decided against that since I have never had VT or VF or any other type of cardiac arrythmia (except for non-symptomatic PVC’s which I was born with).
I believe that I am the lucky recipient of good genetics to begin with, but also I am highly motivated now to take better care of myself, and know as much as I can about the conditions that I have. I plan to have an echocardiogram in six months to see if the LVEF numbers have improved, and I fully expect that they will have. I give credit to the smoking history for the vascular problems that I have including the cardiac problems. I am a lucky person I think, and suspect that not everyone has the fortunate ability to heal themselves the way I have.
I have asked for copies of my arteriogram and stress MRI records. If you are interested in looking at these I would be happy to share them with you.
The letter ends .
Dear Mr Weigel
Yours is an extremely interesting story told in a most scientific manner.Thank you .
It gives me great insight , how a human vascular system can transform when confronted with natural disasters like multiple blocks on its way .A flowing river will definitely reach its destination however bizarre the path it takes . Human biology is vested with vast reserves of genetic building blocks put on sleep mode. While billions of dollars are being pumped into do research in human angiogenesis we have tuned a blind eye to the vast net work of natural collaterals.
Our clinical experiences also tell the same thing . In chronic total occlusion majority of patients would develop good collaterals if only we do not tamper the main vessel .None of scientific studied available has proven opening CTOs (Chronic total occlusions) has improved the clinical outcome .
Regarding the guidelines for revascualrisation , I am yet to come across a standard scientific guidelines that includes the extent of collateral circulation as one of the determinant for need for revascularisation !
I will definitely use your case study for the benefit of so many patients ! I always feel , a properly interpreted experience , even from a single patient can make a tremendous impact in the growth of science .
Thanks again for sharing your personal health issues !
Human coronary circulation stands unique among others as it is a life-sustaining circulation.It is considered a great medical achievement to visualise the right and left coronary artery system by coronary angiogram. Actually what we see is only a fraction of the surface area of coronary circulation . The surface area of epicardial coronary arteries constitutes less than 5 % of entire coronary vascular tree .
This is the reason normal coronary angiogram can never mean normal coronary circulation !
This huge gap in our perception is the single important factor that explains the vagaries of modern coronary care .
This also make any coronary scenario a reality .
“A patient with normal coronary angiogram getting a myocardial infarction the next day and a severe triple vessel disease living comfortably with medical management”
So , it is essentially a false sense of scientific accomplishment by the cardiac scientists at least in the of coronary circulatory physiology.
There are innumerable channels of micro vessels traversing across the heart, sharing , bridging , branching, penetrating and perfusing the muscle mass.They can be anatomicaly patent , physiologically non patent .They can be recruited by hemodynamic stress . It is also influenzed by favirable growth milleu and hormonal and neural stimuli.
What determines the extent of these invisible circulation ?
It has been our traditional teaching ( without much evidence of course !) coronary collateral circulation is not effective to support blood flow during exercise . This fact has been disproved many times . Coronary collateral circulation was indeed useful in limiting damage in ACS and relieve symptoms in stable angina.It helps in reverse remodeling and provided electrical stabilty as well in post MI population.
Still the concept was alienated and made totally irrelevant in the interventional era . Many cardiologists found well-developed collateral’s as an interference to their expertise and ego since it has a potential to alter the indication of PCI.They continue to have strong scientific conviction (Pseudo ?) that man made collaterals must always been superior to God made collaterals !
Whenever some credible reports emerge about collateral circulation being equivalent to revascularisation procedure , these concepts were prematurely buried for some reason.
In the last decade there was a concern about performing PCI in patients with well-developed collaterals .The argument was , they tend to develop early stent occlusion and restenosis . It was a genuine query raised by few thought leaders in the field as collateralised vessels suffer from low flow states after PCI , if the pre -existing collateral continue to function.
But then , few studies countered this , and said PCI is safe and in fact may fares well in patients with extensive collaterals .
In these studies interventionist’s argument looked amusing ! as they seem to define a successful PCI as not only to open the occluded vessel but also make sure to close all functioning collaterals .(What a a pity for our natural biological angiogenic forces which had worked and grown meticulously for months!)
Cardiac science in the current format, makes the future look bleak for coronary a collateral circulation .With early PCI becoming a norm we will never ever allow the natural collaterals to grow , and even the established collaterals will have to face a stiff fight for survival with sophisticated coronary interventions .
Competing interest in the filed of coronary collateral research
While the basic scientists want to grow collaterals with angiogenesis , stem cells etc interventionists continue to indulge in rampant angioplasties which will suppress collateral growth.
This implies we will struggle to establish the true importance of coronary collateral circulation .
Final message
Can it be an effective form of revascularisation ?
My personal inference is coronary collateral circulation “would and should” have a definite role in at- least some of the subsets with chronic coronary syndromes. If we think otherwise . . . it’s against the principle of natural biological science .
A good collateral system with optimal medical management can save not only our patient’s lives but also their hard earned currencies !
Reference
Here is a rare article in European heart journal that discuses coronary collateral circulation . Let us welcome such wonderful reviews which keep the interest alive on the filed.
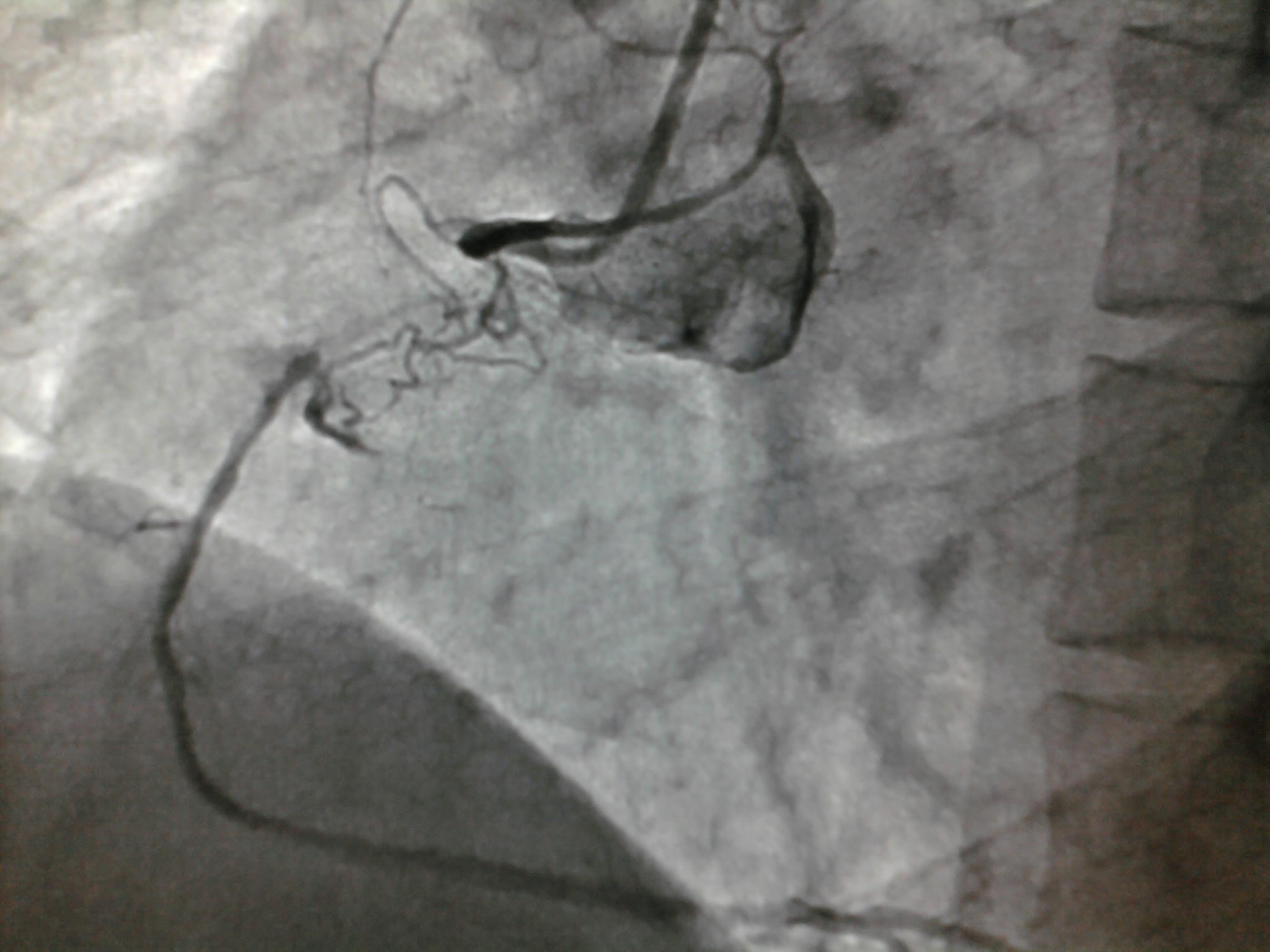
Thousands of coronary angiograms are done every day. Cardiologist no longer get excited to see exotic coronary lesions .Still , some images can be striking and dramatic. Here is an angiogram from a middle aged man with stable angina , who was one among the routine early morning diagnostic studies in our cath lab.
Who chopped the neck of this LAD ?
How this man was able to fill up the distal LAD almost completely? (With a complete cut off right in the neck of LAD )
Are you sure there is antegrade flow ?
Do you get any clue ?
Can a trickle of ante grade flow sustain a TIMI 3 FLOW ?
Or is it a very efficient instant collaterals from LCX ?
Yes . The first one is right . An almost invisible antegrade channel doing a exemplary job !
How is it possible ?
Realize an important fact . The distal flow beyond an obstruction is not primarily dependent on degree of obstruction but the status of the distal vascular bed . If it is normal even a hair-line patency can profusely perfuse the distal myocardial segment. This is what is happening to this man with a stable angina and perfectly normal micro vascular bed.
Lessens from this Image.
Do not get fooled by the lay man’s logic. Realise there is no simple relation between the degree of obstruction and degree of blood flow impediment.It can be linear , curvilinear , or even inverse depending upon the evolution and timing of obstruction , number of lesions , presence or absence of collateral support , finally and most importantly the integrity of microvascular bed .
The distal vascular bed drops its resistance drastically once it senses the problem in proximal segment . This is based on Bernoulli principle and is akin to how a garden hose pipe can simply increase the velocity by tightening the nozzle.*
* The garden hose analogy is a gross simplification of complex factors that determine coronary blood flow.But it effectively clarifies a point ie coronary blood flow is least dependent on coronary stenosis (until very late stages)
**Note further : This hemodynamic principle may not apply in acute occlusion as in STEMI , where acute obstruction often has a linear relationship with the quantum of blood flow.
By the way what happened to the above patient ?
Since he had significant angina there were no debates regarding management. He is posted for elective PCI this week-end .(We can’t get a stent just like that unless it is a real emergency .Ours is a Govt hospital !)
What is your take . Is it a going to be tough cross ?
I feel so , but my colleague Dr Gnanavelu strongly differs !
Coronary collateral circulation can be termed as one of the mysterious circulation in our body.Cardiologists generally do not give much importance to it and some interventionists even ridicule it ! . But , God has given it , with a purpose. He adds a riddle though ! .Collaterals grow in almost every individual when obstruction occurs gradually ( chronic coronary syndrome ) but only in a few , it will open up during a real emergency like ACS !
How and why , only few of us can recruit coronary collaterals during acute occlusion ?
God blesses acute coronary collaterals only in selected few , who are on the right side of his good books .This can be the other name for our destiny !
Role of coronary collateral circulation in acute coronary syndrome.
Limits infarct size and volume
Promotes salvage
Converts q MI to non q MI
Prevents Unstable angina from becoming MI
Prevent primary VT and VF*
All of the above can be vital in saving a life . Even as we realise 30 % of STEMI do not even reach hospital , it seems certain men and women with early collateral recruitment will never fail to reach the hospital alive
Is there a simple method to identify people who are blessed with acutely recruitable collaterlas ?
I am afraid it is almost equal to asking for a glimpse of GOD !
Wait . . . when we were on cath lab few days ago a stunning phenomenon happened that could pave way for identifying potential acute collaterals in any human being. Follow this site . . .the details will be posted !
Coronary collateral circulation is probably the most poorly understood circulation than any other.This is ignorance at it’s best , in spite of the life saving potential of this circulation. A popular (mis )perception is coronary collaterals can support only resting blood flow and it would struggle to compensate at times of exertion. This is based on few case studies and not based on large , authentic scientific data.
Does this reasoning mean , coronary collaterals can never / ever be complete ?
If we believe so . . .we are grossly underestimating the power of nature .(In fact , mankind was humiliated by the nature time and again !)
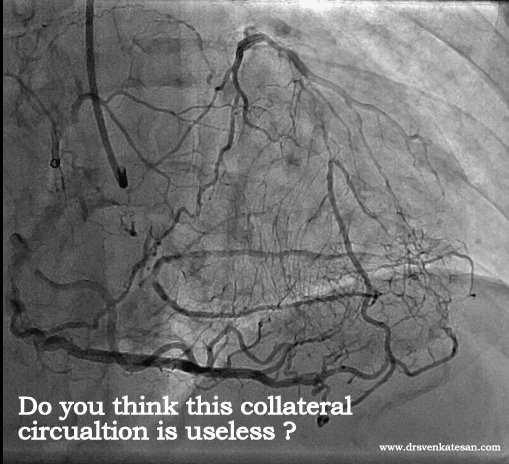
Lessons from a unique patient we have encountered.
Here is an example of total LAD/LCX occlusion with good collateral from RCA. He was having stable angina on medical management . This patient was not only asymptomatic and was also negative for exercise stress test at moderate work load .
There was an intense debate about the management when this angiogram was presented in the cath meeting .
Most of the cardiologists believed so ! But they had no answers why his stress test was negative.
The other argument for CABG was one can not allow a patient with a functionally single coronary artery (RCA) However good is the collateral circulation.This at least has some logic. not the first one !
One more suggestion was to quantitate and map the real extent of ischemia by PET scanning and then decide about revascularisation.
One critical opinion was , since he was doing well with medical management what was the need to do coronary angiogram at all ?
Any answers . . .
He ultimately went on to receive CABG (By popular opinion ) , but the point here is the collaterals were good enough to support exertion.We have documented quiet a few similar patients with collateral circulation supporting exercise.
What happened to the collaterals and (of course ) the patient after surgery ?
I will post you the curious story soon . . .
Final message
Coronary collateral circulation , if well developed can provide hemo-dynamically useful support even at times of exertion *
* The existing literature is biased against this concept. It generalizes all grades of collaterals into a single entity. It is better if we spend more time to understand the nuances of coronary collateral circulation .
This is the message from our observation. Do not ever believe whatever is published as facts in scientific literature. Observe, analyse , create your own inference , and concepts. Mainstream cardiologists would brand it unscientific , Simply ignore it . Many times it is rewarding to our patients.
Total coronary artery occlusion is a common finding in CAD especially in chronic stable angina. Normal coronary blood flow is 5 % of cardiac output that amounts to 250-300ml/mt.At an average heart rate of 70/mt , each beat injects about 5cc blood into the coronary circulation.This is shared between two coronary arteries. This means , only few CC (2-3cc) of blood enters each coronary artery with each cardiac cycle .
When one of coronary artery is totally occluded what happens to the coronary
blood flow ?
A.Total coronary blood flow can be be maintained normal at rest as it forms only about 5% of cardiac output (or it is only slightly reduced )
B. It is believed , the unobstructed coronary artery could receive the blood meant for the contralateral coronary artery. This possibly explains the increased coronary artery diameter in the non obstructed artery.
C. It’s nature’s wish , that the contralateral coronary artery shall share 50% of it’s blood through collaterals if available.
D.If collaterals are not formed it , the unobstructed coronary artery may be over perfused with double the amount of blood flow.
E. Some times , the collaterals steal much more than what the obstructed coronary artery deserves and make the feeding coronary artery ischemic. This is many times observed in total RCA occlusion with well formed collaterals from LAD/LCX.
F.The collateral flow in CTO also depend on whether flow is directed from LAD system to RCA or from RCA -LAD system. The LAD is better placed to assist RCA than vice versa.This is for two reasons.1.LAD blood flow is higher than RCA so it can share it.2.The driving pressure is more from LAD -RCA , as RCA can receive blood flow even during diastole .
F.During exertion , the coronary hemodynamics become further complex.The collateral’s are traditionally thought to be less than adequate during times of exercise.But it is more of a perception than solid scientific data.This rule may be applicable in only certain group of patients. We know CTO patients with very good exercise tolerance who have documented collateral’s.
G.Collaterals can be either visible or invisible by CAG. The strength of collateral circulation is not in it’s visibility but it’s capacity to dilate and respond to neuro humoral mediators at times of demand. Currently , there is lot to be desired regarding our knowledge about the physiology of visible collaterals , no need to mention about invisible collaterals !
Final message
The above statements are based on logics and observations .
Is it not a irony in cardiac literature , where thousands of articles are coming out every month to tackle totally occluded coronary artery(CTOs) , there is very little data regarding the coronary hemodynamics in chronic total occlusion . How does a patient with CTO can manage a active life with only one functioning coronary artery ?
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.
















{kind=link}
{kind=link}
{kind=link}
{kind=link}