We know q waves are not synonymous with Infarct . It just represents electrical activity going away from the electrode.This is why it can occur even in physiologically in many leads.
Non infarct Q wave can be recorded with
- LVH
- Fibrosis
- Fluid/Air in beneath the recording lead
- Thick chest wall/pericardium (More often Poor R wave )
When a chamber enlarges (Any chamber ) it is brought near the chest wall the electrode may pick up the intra cavity potential that is recorded as q waves .
(The q wave in V5-V6 in severe volume overload of LV may represent LV cavity potential )
Similarly qR complex in severe RV enlargement in V1 represent RA cavity potential.Right ventricle is anatomically a difficult chamber to understand. It is located anterior below the sternum the inferior and posterior aspect of the RV is facing the diapharagmatic surface
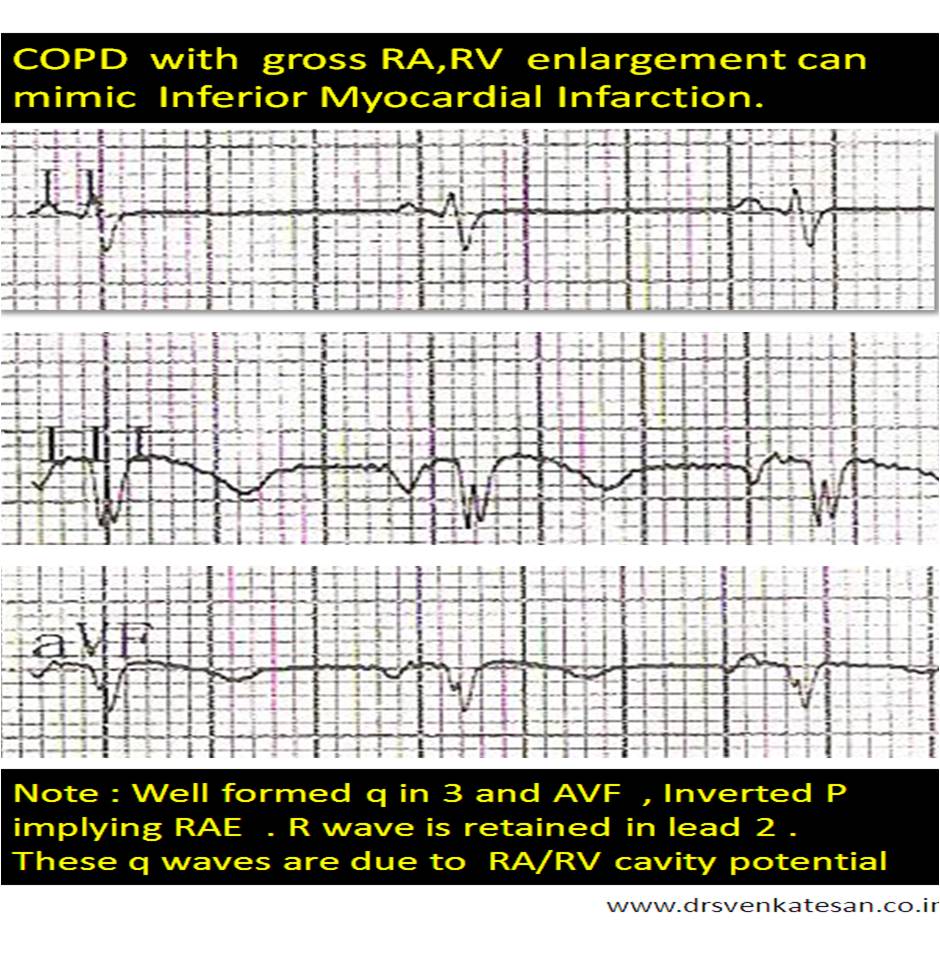
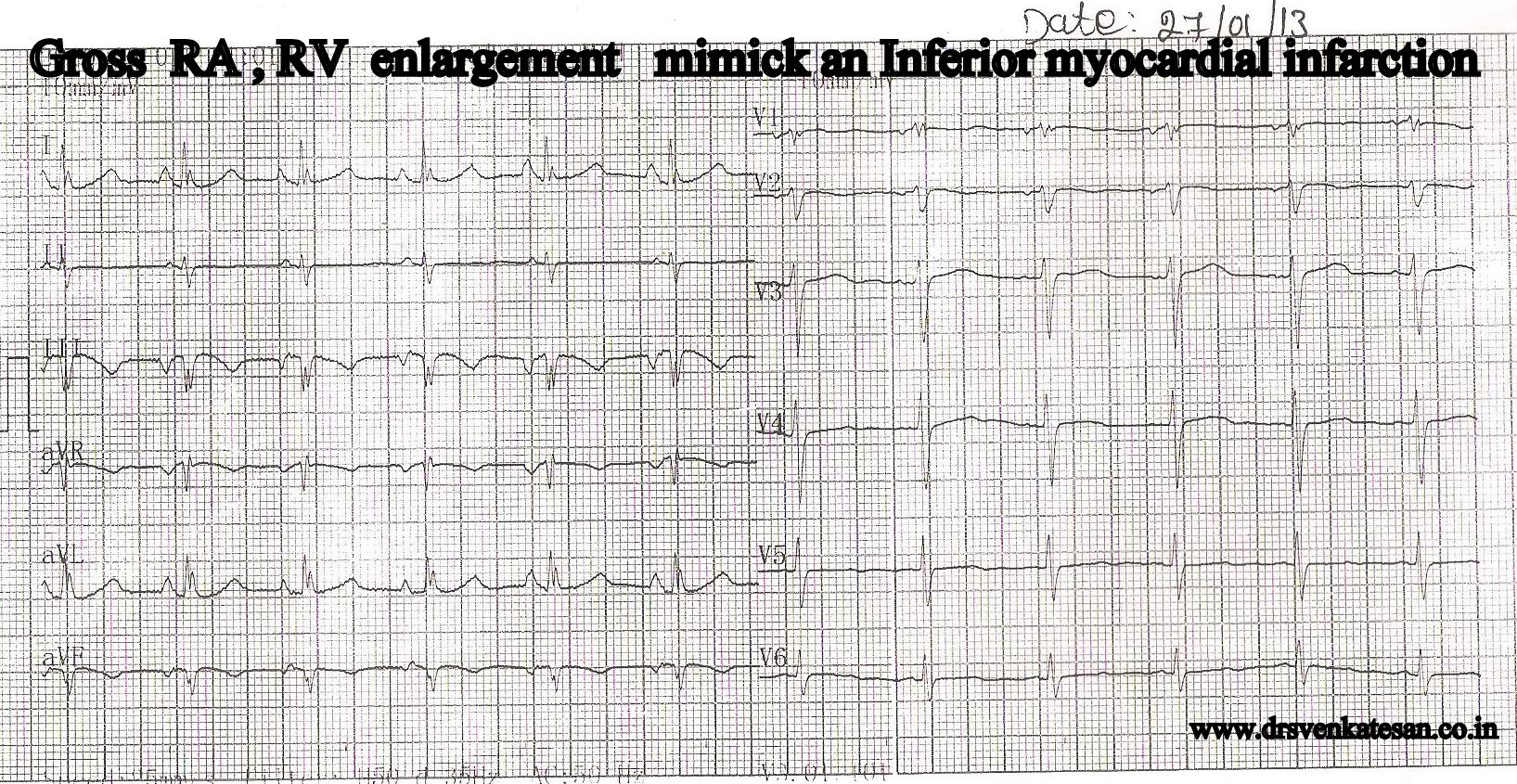
In huge RV enlargement , RV cavity potential or( even RA ) can be picked up by limb leads . While cavity potential is well picked up by unipolar pre-cadial leads , it is uncommon for limb lead record intracavitory potential. However this patient , who was diagnosed as inferior MI by a resident , turned out to be a clear case of severe pulmonary hypertension due to COPD .
Final message
One more differential diagnosis for inferior MI in ECG exists. A grossly dilated RA, RV due to COPD with severe pulmonary hypertension.




Leave a comment