A tense anesthetist calls for help !
I had an unusual cardiac consult last week .A middle aged man who was to undergo routine ortho surgery wanted a cardiac clearance.
It was a through and through fracture of clavicle , why do they need a cardiology opinion , it seemed a simple procedure I asked over phone
The anesthetic fellow who was in charge of the patient told me ,”There is a wire just going parallel to the clavicle sir .I believe it is pacemaker lead” I agreed to see the patient immediately
This was the X-ray
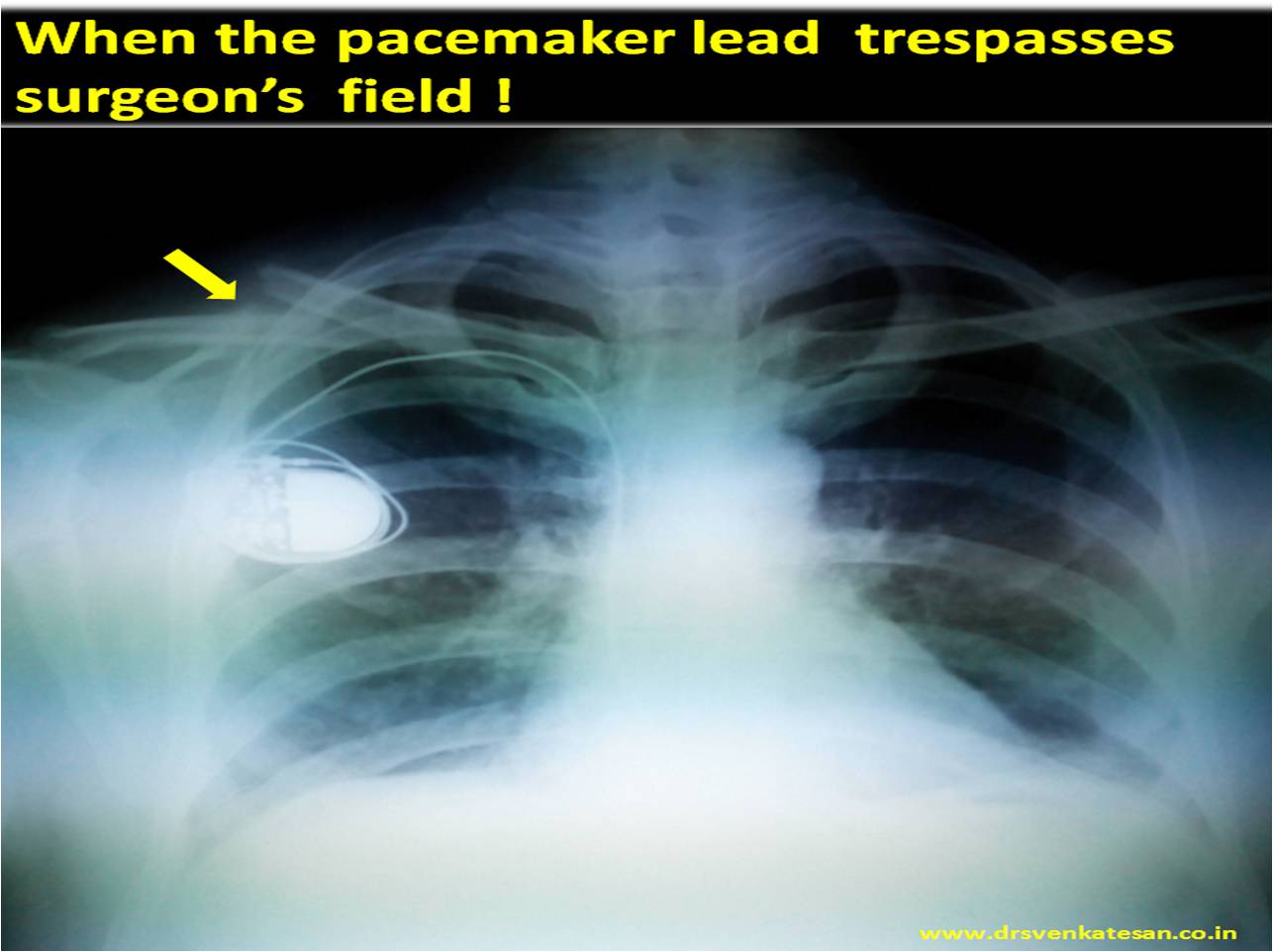
It was obvious why they got tensed up as the pacemaker wire criss -crossed surgical field . His ECG showed own rhythm of 80/minute but occasionally VVI pacemaker was capturing his ventricles.
I suggested
General precautions
- Strict Intra-operative ECG monitoring
- Keep another temporary pacer ready .
- Hold a cardiologist on call and pacemaker programmer on site.
- Surgical field kept small with minimal manipulation .
- Issue of cautery : Free to do as long as it’s bipolar and good earthing plate.
- Ensure the cautery is applied in one or two second pulses with a gap of 10 seconds pause in-between
- Wiring the clavicle – Signal interference are very rare as the wires are inert
Use of magnet in such situations (Link to magnet and Pacemaker)
Keeping a magnet over the pacemaker generator removes the pacemaker sensing function and is an option if prolonged electrical interference.
*Caution : Response to magnet can be quiet variable .Should be done only with cardiologist supervision.
What happened to this patient during surgery ?
Nothing alarming.When anesthesia was induced he was entirely on pacemaker rhythm . limited cautery was used with ease. Patient tolerated well.
Final message.
One need not panic when a pacemaker patient is taken up for non cardiac surgery .It is not a major issue .Few precautions are required .
Read a related article in this site .Electrical cautery in pacemaker patients.
Reference





Leave a comment