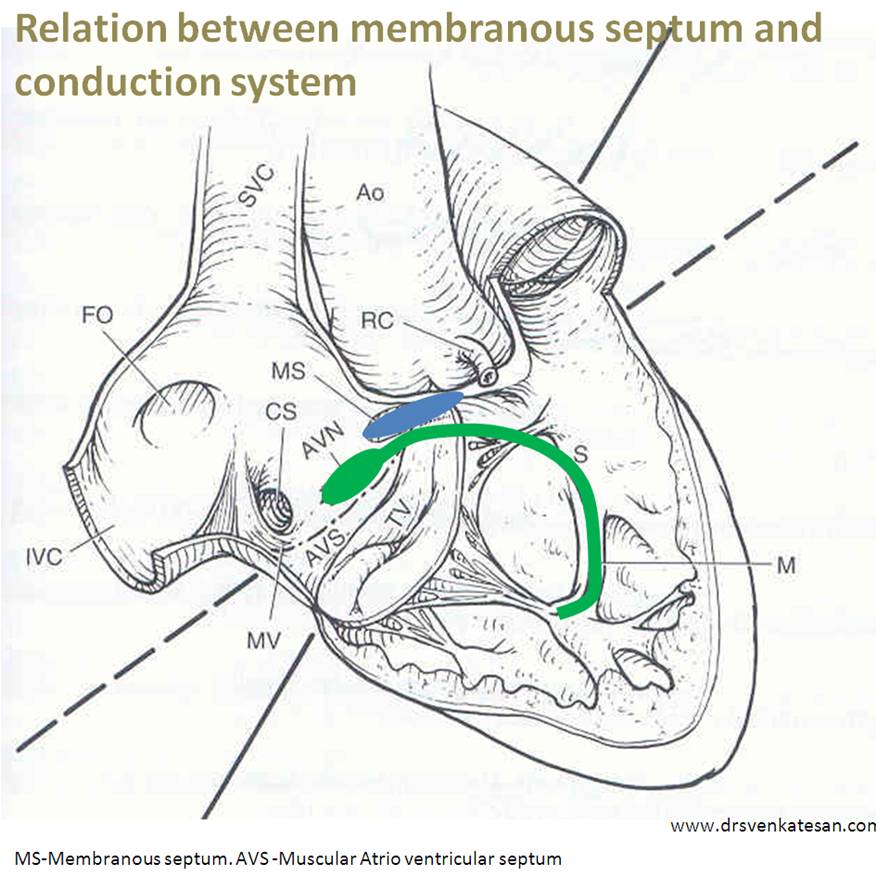
Failure of enocardardial cushions to separate and reach the predesignated destination ie right and left AV valve is the basic embryological feature in AV canal defect .This brings whole AV ring down and stretches the distance between the semi-lunar valve (especially aortic) with that of LV , thus elongating the LVOT into a classical goose neck deformity.The defect has a profound impact on how the AV node and its branches penetrate the ill-formed AV junctional tissue and fan out into the ventricle. There are four basic issues that are responsible for the various conduction defects in AV canal defect.
- Postero- inferior displacement of the A-V node is the key abnormality .
- Hence AV node penetrates the ventricle at the level of crux which is abnormal .This results in short his bundle (AV node short of compressed with His early direct origin of the left bundle branching)
- Left bundle branching system by itself is also abnormal with hypoplasia left anterior bundle branches.
- Right bundle branch is relatively long and elongated
Physiological effects
- Prolonged PR interval (50%)
- QRS axis shift can be extreme right or left , but superior direction is a rule .Typically its around -180 . Left axis deviation is distinct in downs syndrome (Counter-clock wise rotation q in lead 1 and AVL ) .It should be learnt , the ECG features (due to anatomical defects in AV conduction system ) can be be easily modified by the hemodynamic stress of ventricles due to associated conditions and classical pattern may non exist )
- Surprisingly high grade AV blocks are rare (“viz a viz” LTGV )
Electro-physiology
Short HV interval is documented in AV canal defects inspite of prolonged PR due to small his bundle length.
A large Inlet VSD , simply takes over the place meant for the conducting system and its pushed down and out
Reference




Leave a comment