One may recall some stunningly simple facts from our high school biology classes that every living cell needs energy on a moment to moment basis.
Blood vessels which take care of the vital organ’s energy supply also need the same blood (Nutrients /Oxygen) for its own survival.
Coronary arteries carry about 250 ml of blood every minute , 24/7 supplying ATP enriched fuel to the heart.
Who is feeding these delicate vessels which carry on this life-sustaining work ?
It is easier to assume the three layers of the blood vessels which are bathed with blood would never suffer from Ischemia. Reality is different .Blood vessels do suffer from Ischemia.We do have evidence medial necrosis, plaque instablity , fibrous cap disruptions may be due to a vascular insult or vessel wall energy deficit.
The much debated entities like endothelial erosion and dysfunction are often atributed to mechanical stress , sympathetic spike , or smoke . This may be a virtual guess as no one knows what causes these. It could well be a patchy Ischemia due to endothelial perfusion defect from within or a vasavasoral dysfunction from outside. Coronary ulcers some times mimic gastric ones and guess the cause ! yes it is mucosal ischemia !) *Ischemic ulcers in GI tracts can be common (Schweiz Rundsch Med Prax. 1993 Jun 15;82(24):709-13)
Image source http://www.wikidoc.com
How does coronary artery gets it blood supply ?

Busy cardiologists have no time to worry about nourishment of the coronary arteries . . . even as they play inside with unlimited arms and ammunition.We leave it to our basic scientists.
So , how does coronary artery gets its blood supply ?
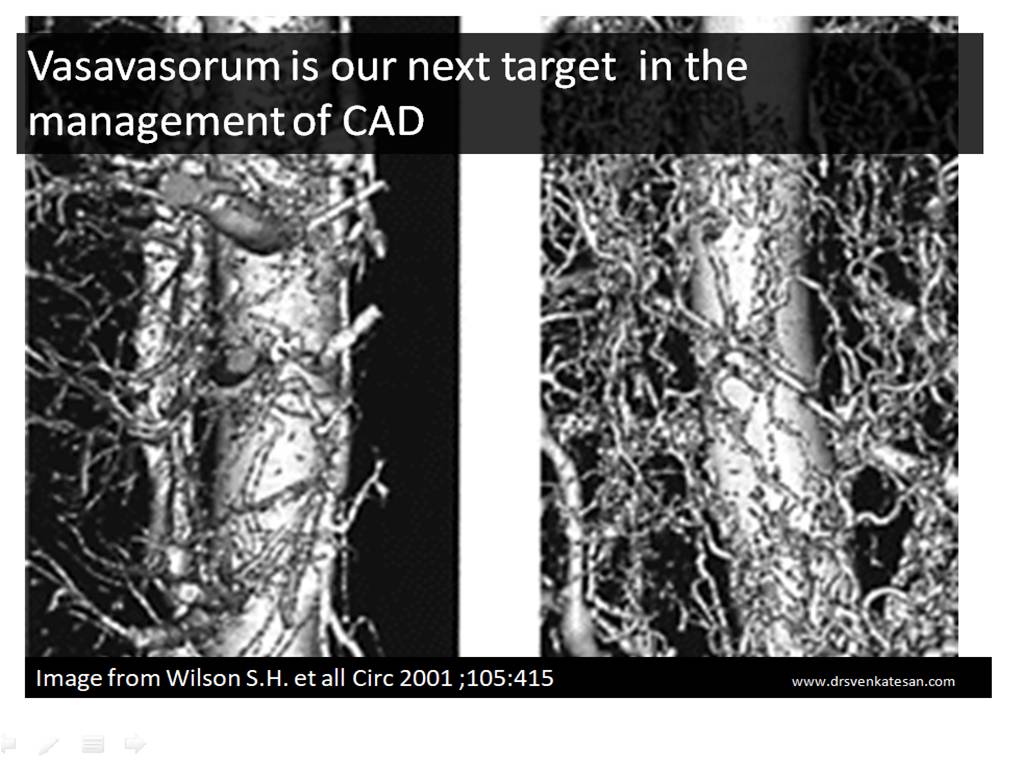
The easiest answer is, blood supply to coronary artery is taken care by a vast network of micro vessels called vasa vasorum(VV) . Of course, the inner layers of Intima and media do get some nourishment by the flowing blood as mentioned earlier.No one really knows the quantum of blood flow that perfuse within the planes of coronary artery.
*By the way , does the vasa -vasorum comes from extra-coronary source or from the same parent vessel ? (I think the answer is both ! will try to find out!)
It should be noted Vasa vasorum is well developed only in large arteries. VV has one more important function ie to drain the metabolic excreta from the walls of blood vessels. This function could never be taken lightly as failure to do so will result in vascular wall edema in acute setting or thickening In chronic setting.
Does coronary arterial tree goes for necrosis in STEMI ?
There is some evidence , when acute total occlusion happens in an epicardial vessel , not only the myocardium is ischemic , the entire distal coronary vascular tree becomes vulnerable. The ischemic time and resistance of coronary macro vs micro vasculature is currently not known. It is expected to show significant variation . We know ,one of the important mechanism of no re-flow following PCI is due to microvascular damage(Non thrombotic)
Many times we fail to realise myocardial viablity and micro-vasculature integirty are two different things. ! This questions the concept of reperfusion based on the status of viable myocardium alone.This we have experienced in many patients as myocardial viability doesn’t guarantee you full recovery from LV dysfunction as microvasculature may recovery may lag behind or never restored (Permanent vasa-vasoral damage ?)
What is our knowledge base about exclusive pathology of coronary vasa vasorum ?
Do you know, ectasia, arteritis, aneurysms and external band like compression of coronary artery all are related to some sort of vasa vasoral dysfunction ? We are not yet clear whether atherosclerosis really involves the vasa vasorum.(Takayasu does it for sure ! )
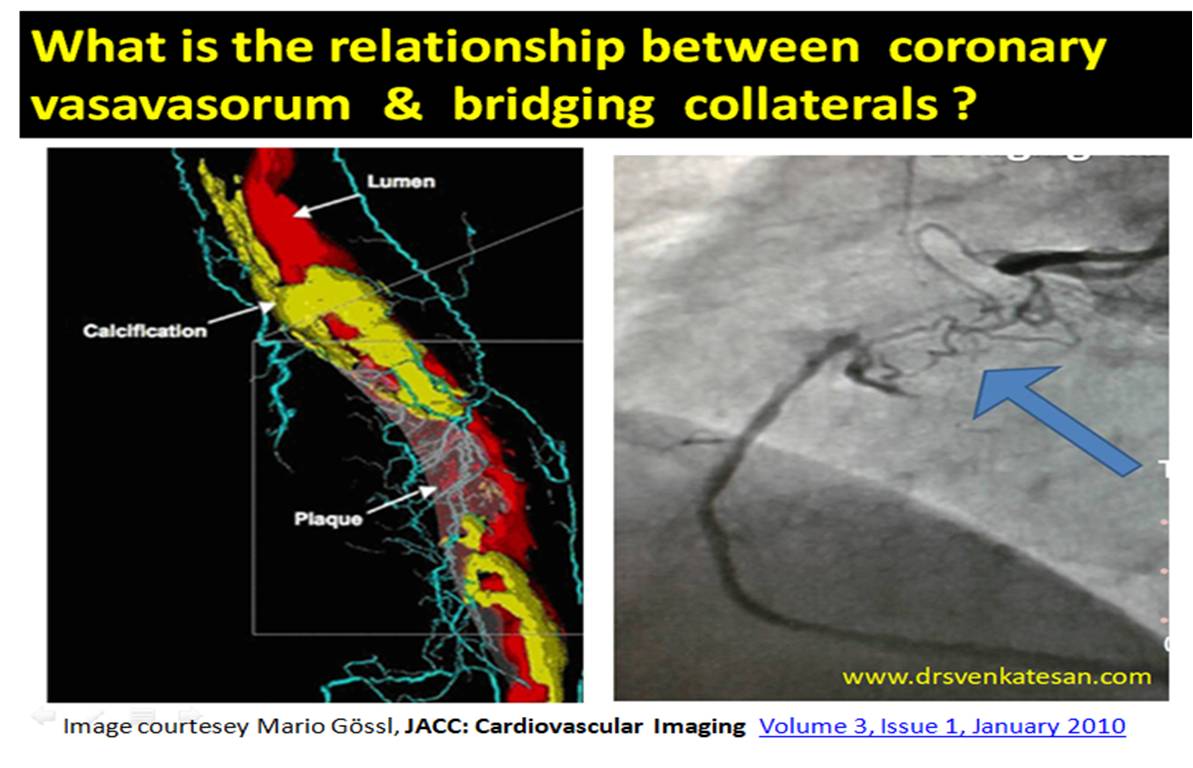
What is the relationship between vasa vasorum and coronary collaterals ?
It seems to me , many of bridging collaterals are nothing but extension of vasa vasorum and ultimately arise from epicardial coronary collaterals. (Some youngster’s take up this topics for research)
Why is high pressure post dilatation a double-edged sword ?
It’s often thought , larger the lumen its better. Need not be. These are all some questions which we don’t have an answer.
What is the radial pressure exerted by coronary stents on coronary trans -arterial perfusion ?
Does coronary artery go for Ischemic necrosis with high pressure Inflations ? As such there is no published evidence . By the time we wait for published evidence enough number of coronary arteries might get damaged. So try to use common sense .
Relationship between delayed Mal-apposition & vasa vasoral damage
It is very likely ,the so-called endo-leak which is quiet prevalent in aortic interventions is could be seen in coronary arteries. We are not recognising it. It could be same as Intramural hematoma in certain subsets.
Meanwhile, self expanding stents with good radial strength has made a come back .While it may prevent a mal-apposition ,has a potential to stress the vessel wall (Radially) and in the process interfering with perfusion.
Does Vasa vasorum promotes Atherosclerosis or negates it ?
hehttps://www.hindawi.com/journals/bmri/2014/701571
The irony is, while de-novo vasa vasorum is the life line for coronary arterial nutrition, neo-vascularisation is problematic .Then how to selectively promote good vasa vasoral growth and avoid the pathological network that promotes adventitial nodular degeneration ? This is were the curious basic scientists and casual cath lab guys need to interact.What is positive remodelling ? (Often referred to the famous concept of Glagov ) How can we promote it to maintain good luminal diameter inspite of large burden of atherosclerosis by manipulating the vasavasorum.
Final message
Cardiologists are ahead of others in many cutting edge technology. There is no two opinions about it. Who can repair a live beating heart without stoping it for a moment ? Still, there is a whole lot of coronary Ignorance waiting to be explored. Blood supply to coronary artery is one such area to be decoded.This will have larger implications as Vascular healing , plaque survival and growth depends upon vasa vasoral integrity as well as neo vascularisation.
While , metallic management of CAD seems to be the order of the day as it tends to give an instant fix .My guess would be medical sense would ultimately prevail one day with controlled vascular aging and natural ,pharmacological ,biological repair of cells will prevail over temporary patch work in cath labs.
Reference
What is the role of newer Imaging and OCT in visualising Vasa vasorum ?
It is going to open up new avenues in our coronary vision.
(Kensuke Nishimiya European Cardiology Review 2017;12(2):121–3)