Here is an uncommon story of a patient with palpitation,SVT , Troponin +ve, and suspected ACS.
Palpitation in ER ⇒ {Tachycardia +Troponin positive ≠ ACS}
Mechanism of troponin elevation following any SVT
- At high heart rates (>200) myocardium is subjected to non-Ischemic mechanical strain & squeeze. Minute amounts of Troponin is let out like a myocardial juice into the circulation (Like atrial natriuretic peptide release which causes polyuria during AVNRT)
- Tropinin releases have been shown to correlate with both heart rate and duration of ST depression (Subendocardial strain /AVRT left lateral pathways)
- Short diastole induced low coronary perfusion pressure and a true transient (but insignificant) Ischemia
- Finally, SVT (especially in the elderly) is a natural “exercise stress test” equivalent, ST depression with Troponin positivity is a true marker of significant epicardial CAD
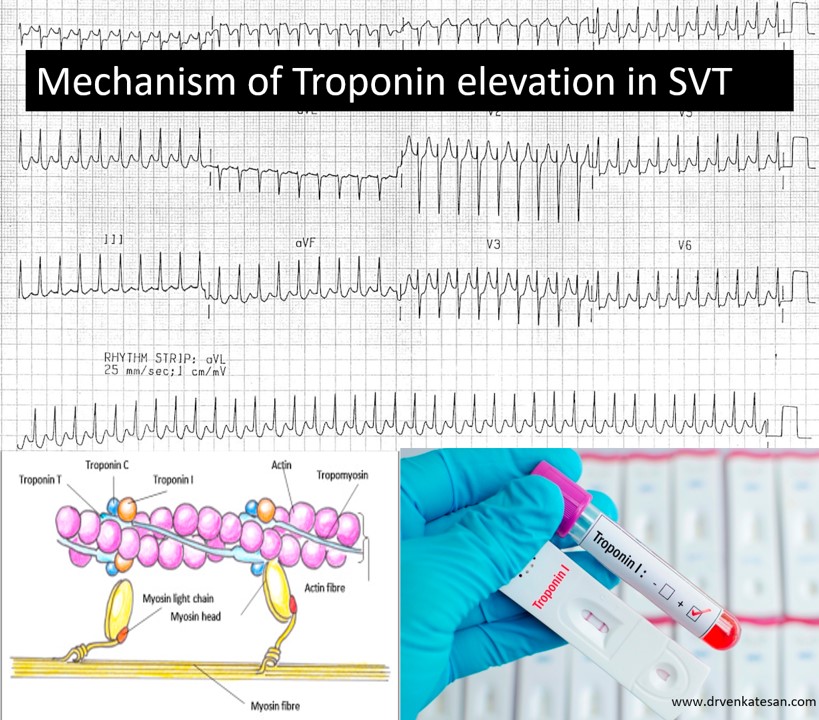
ECG courtesy https://litfl.com/st-segment-ecg-library/
Significance
False alarm of ACS is the most important issue. (Except one study which showed a different conclusion Chow GV, Prognostic significance of cardiac troponin I level in hospitalized patients presenting with supraventricular tachycardia. Medicine (Baltimore) 2010;89:141–148. doi: 10.1097/MD.0b013e3181dddb3b. [PubMed]
Note: If AVNRT occurs with aberrancy, or AVRT presents as antidromic tachycardia with a wide qrs tachycardia the confounding effect is perfect as it can no way be differentiated from true Ischemic VT or atrial fibrillation.
Final message
It is no ER room secret that a single spot Troponin value has lost its credibility considerably in segregating ACS from non-ACS conditions. It is falsely elevated in a long list of cardiac and noncardiac conditions. It is a worthy point of learning, among the cardiac conditions, the commonest cause for false elevation is during any tachycardia. This should be kept in mind. Because a patient with chest pain who present with benign palpitation due to prior SVT (Arrival ECG could be normal) a false raise can trigger a chain of inappropriate reaction that may land the spot even in the cath lab.
Postample
In spite of these limitations, non-diagnostic ECGs, we expect Troponin and CPK to guide us in chest pain screening. We now have added one more marker, high sensitivity Troponin Assays. Let us believe, it doesn’t add to more confusion. I think the main purpose of these biomarkers in the future, would be to arrest the habit of using cath lab as triaging place for chest pain instead of ER room. (A brief review from ACC https://www.acc.org/latest-in-cardiology/articles/2017/08/07/07/46/a-brief-review-of-troponin-testing-for-clinicians)
Reference
1.Troponin elevation in supraventricular tachycardia: primary dependence on heart rate. Ben Yedder N, Roux JF, Paredes FA Can J Cardiol. 2011 Jan-Feb; 27(1):105-9. [PubMed] [Ref list]
2.Kanjwal K, Imran N, Grubb B, Kanjwal Y. Troponin elevation in patients with various tachycardias and normal epicardial coronaries. Indian Pacing Electrophysiol J. 2008;8(3):172-174. Published 2008 Aug 1.
3.Carlberg DJ, Tsuchitani S, Barlotta KS, Brady WJ. Serum troponin testing in patients with paroxysmal supraventricular tachycardia: outcome after ED care. Am J Emerg Med. 2011;29:545–548. doi: 10.1016/j.ajem.2010.01.041. [PubMed] [CrossRef] [Google Scholar]



