Here is a pleasant surprise, a collectors issue of NEJM year book 2023, is made available free (even for non subscribers, in its website) .It is fascinating to know how fast the Internal medicine has grown. For the busy cardiologists, this will a be refreshing reminder, that there are other important organs and specialties do exist in medicine , with equal breakthroughs and Innovations.
It is indeed an amazing , whirlwind tour of medicine for all those who see medical science as single holistic specialty. It has articles, ranging from from simple clinical studies on postpartum hemorrhage (E-MOTIVE study) from deep inside Africa by Melinda Gate foundation, to Dupilumab for COPD, a stunning monoclonal antibody inhibitor of IL-4 for COPD exacerbations. Shortening tuberculosis treatment with a strategy involving initial treatment with an 8-week Bedaquiline-linezolid regimen (TRUNCATE-TB study) is also a revelation.
Of-course, the mandatory cardiac topics do find a prominent place including the currently omnipresent drug GLP agonist Semaglutide for HFpEF (STEP-HFpEF study). Baxdrostat, an Aldosterone synthase antagonist for treatment-resistant Hypertension, appears promising (BrigHTN).
Final message
However, the crowning glory among all articles appear towards the end of the document, titled Combating misinformation as a core Function of Public Health.
Let me share the link to this PDF document here. Hope it allows open access and there are no copyright issues. Notable articles of 2023 from NEJM .
High-density lipoproteins (HDLs) represent a class of lipids, very heterogeneous in structure, composition, and biological functions .The density is between 1.063 to 1.210. It has at least 5 sub-types. Normal HDL level in blood should be above 35mg (50-60mg Ideal). When it goes beyond 60 there is not much benefit to accrue and also some surprise findings are there.(Article will be linked soon)
We know ,HDL carries free cholesterol from peripheral cells, including macrophages and endothelial cells. After reaching the liver, HDL receptors in the hepatocellular surface, metabolize it into bile acid or neutral lipids, which are excreted as bile and feces. This is the much famous Reverse Cholesterol Transport(RCT) and the anti-atherosclerotic effect of HDL .It must be emphasized apart from RCT, it has antioxidant, anti-inflammatory, antithrombotic, and vasodilator actions. Two good reference : One is a book ,that was a surprise .(Review article on HDL)(A text book on HDL )
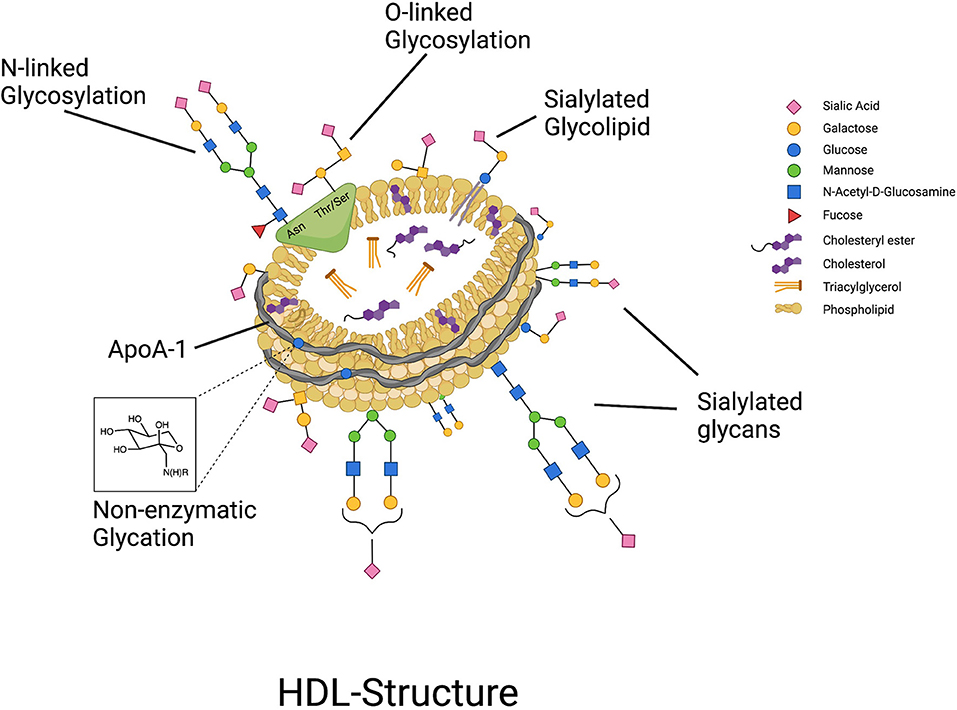
Structure and shape
HDLs are real complex lipids occurring as pseudomicellar, quasi-spherical lipidomes. It has at-least 80 different binding sites for various proteins and ligands. APO A1 is the major apo-lipoprotein which mediates its action.
In one way, it looks like an International Space Station orbiting in the bloodstream, with multiple docking and releasing points. We are far away, from understanding the role and function of various molecules that get either activated or deactivated either in the circulation or inside the cells. Unlike other sub fractions of lipid, HDL evades routine imaging by NMR or X-ray crystallography. This is one of the reasons we find it to understand this molecule fully.
HDL : The untold story !
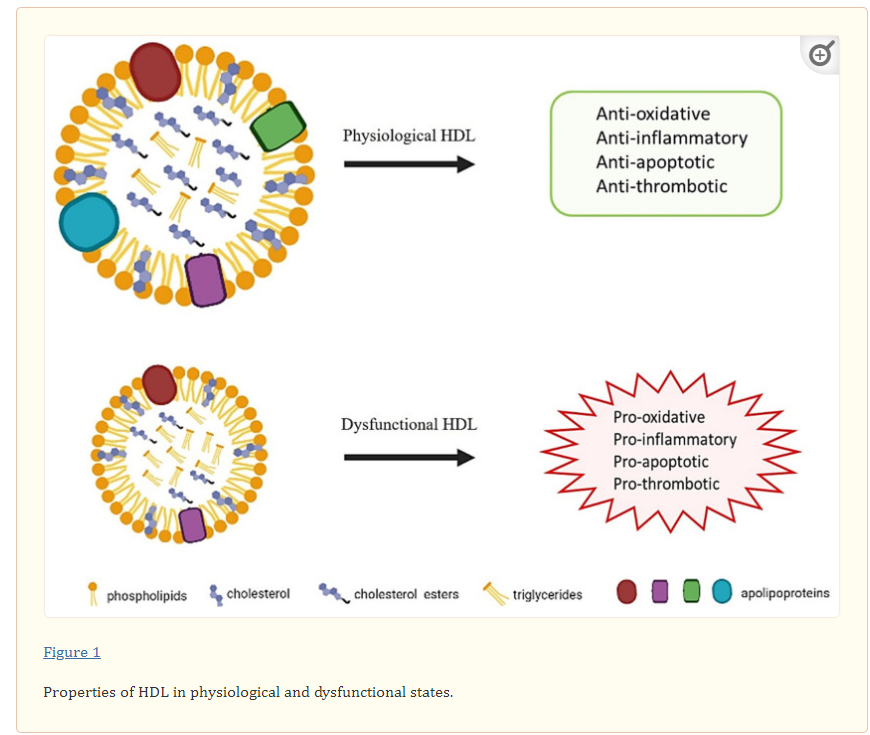
Despite the evidence suggesting a clear inverse relationship between HDL cholesterol concentration and the risk for cardiovascular disease, plasma HDL cholesterol levels do not predict the functionality and composition of HDLs. It can change color from good to bad with a drop of a hatin various clinical situations.
A combination of obesity & diabetes has high chance of pushing this molecule into bad times. There is evidence, (primarily in this setting) HDL undergoes structural changes, and exhibiting pro-inflammatory, pro-oxidant, prothrombotic, and pro-apoptotic properties.(Sounds more ominous than LDL is it not ?)
Glycolysation of HDL
Diabetics results in systemic glycation of all cells or whatever molecule the blood bathes in. We also know the core pathology of diabetic micro angiopathy and basement membrane defects in various target organs are due to this. glycation.
A rigid HDL : The key to HDL function lies not only in its structure but also in the shape. It need to be flexible .It is expected to change its shape like a chameleon, while ferrying the cholesterol to liver. It has multiple shapes to choose from, discoid to double helix , spherical as and when required. A rigid HDL struggles to perform its action. Docking and alignment issues with ApO A 1 and A 2 is also contribute to the molecular dysfunction.
Link between HDL and platelet : We are getting more surprises with the multifaceted nature of HDL. Its been demonstrated HDL degrades PAF(platelet activating facto quicker) . hence ,a dysfunctional HDL can change the hematological milieu to pro-coagulant state. European Heart Journal, Volume 44, Issue 16 2023, 1394–1407,
How to know whether my HDL is functioning all right ?
HDL sub-fractions, APO A 2 are not routinely measured as clinical tool. As of now, there is no practical tests to know it. No worries. If we start thinking about every molecules’ integrity (Just, we have few billions of it ) life will be made miserable. Be-calm, carry on with your work .Trust your HDL, it will remain good for you. Take care of all risk factors and lifestyles that is within your control. This piece is written for the cardiology fellows to understand , the dichotomy between CAD and dyslipidemia.
Final message
*Wemust admit, as scientists we have had little understanding about HDL. Still, to the public we have passed on a possibly erratic message that HDL is a hero in our fight against CAD. This is purely based on, one of its action i.e., RCT.Maintaining HDL level as per guidelines is good, but the reassurance given by that number can be a superfluous.
*Meanwhile, the concept of Non/dysfunctional HDL can not be taken lightly, since there is considerable evidence to suggest it might transform into a hazardous one in an undefined span of time. This explains the poor correlation between dyslipidemia and CAD risk. More comprehensive research is required to progress further in the field of lipid biology.
A cath lab is an “optional accessory” in the management of Acute coronary syndrome (ACS).
True or False ?
Answer
“Without a CCU…you can never, treat any Acute coronary syndrome … while we can treat most ACSssuccessfully without a cath lab “ (If you still got the answer wrong …sorry, no comments)
Best comment
Accessory is ok , but it is “20% foolish” to state cath-lab is optional, it should be mandatory.
What will happen if you happen to thrombolyseWellen syndrome?
Will evolve into STEMI by prothrombotic trigger of lytic agent
ECG will get normalised with clinical stability in some
Nothing happens. ECG will remain same.
Worsen the situation in majority
Will be severely reprimanded by your consultant and peers.
Answer:
4 will be answer for most of us , while 2 and 3 is a lesser, but distinct possibility. I have never seen 1 happen .Whatever is the correct answer , response 5 will always be correct.
What is the criteria to diagnose Wellen syndrome ?
The criteria used to diagnose Wellen syndrome include symmetric and deeply inverted T waves or biphasic T waves in leads V2 and V3 in a pain-free state, plus isoelectric or minimally elevated (<1 mm) ST segment. In addition, the criteria require the absence of precordial Q waves, the presence of history of angina, and normal or slightly elevated cardiac serum markers.
Wellens is a glorified subset of ACS. It can be referred to as an ACS in a confused state of evolution. Most often a critical mechanical LAD lesion is noted. Thrombus, by no means is excluded. This is the reason some times lytics work. Spasm of epicardial coronary artery is also part of the problem. Since Wellens patients exhibit dynamic symptoms akin to their T waves (often in an inverse relation), it is natural that cardiologists are also tentative, especially if these patients have hypertension and LVH as well.
1.How to manage Wellen syndrome?
Majority of Wellens end up as NSTEMI, statistics tells us about 20% of them can be STEMI in incognito mode demanding lysis or emergency PCI. Since lysis is harmful in subtotal occlusion, it is safe to take all Wellens to cath lab and decide thereafter.
2.Is Wellens exclusive to LAD ?
No. RCA and LCX Wellens do occur, making this entity’s perceived unique importance less certain
3.How common is thrombosis in the culprit artery of Wellen syndrome ?
It is generally believed it is more of a mechanical plaque lesion. However by no means, we can say thrombosis do not occur. This is the reason lytics sometimes work , though we argue it as apparent contraindication.
4.Is there a benign face of Wellen syndrome ?
Yes, we believe so. If Wellen presents as evolved Non -Q-MI or as evolved NSTEMI, a term most cardiologist will not agree with existence of such a terminology .(Clinically, stabilised unstable angina also falls under this category)
Final message
It is curious truth, even fearsome STEMI can be effectively managed without knowing the coronary anatomy (with thrombolysis) ,while Wellen’s a lesser emergency demands more urgent knowledge of coronary anatomy .
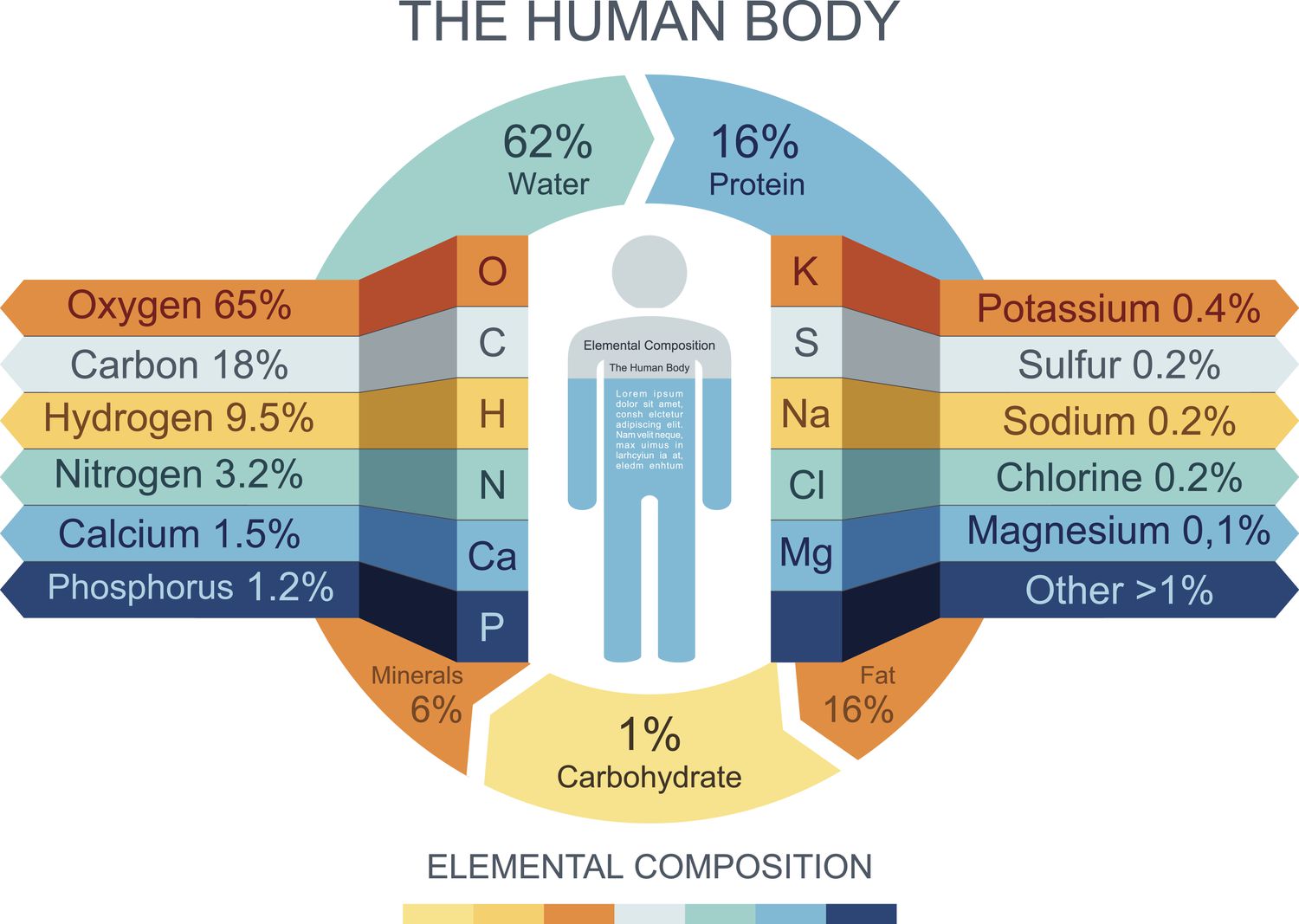
15 % of body weight is fat. (10kg) Out of which just 250 mg of cholesterol is streaming in blood. We must understand fat, lipid and cholesterol are different entities. LDL is obviously a target against atherosclerosis. While the total body fat seems to do little in determining blood cholesterol levels, what is more scientifically shocking is the slope of curve between blood LDL levels and plaque burden is rarely linear. Mind you, LDL constitutes .000025% of total fat. We have many other targets in dyslipidemia like free cholesterol, harmful fatty acids, remnant cholesterol, TGLs, dysfunctional HDLs
LDL is not innocent
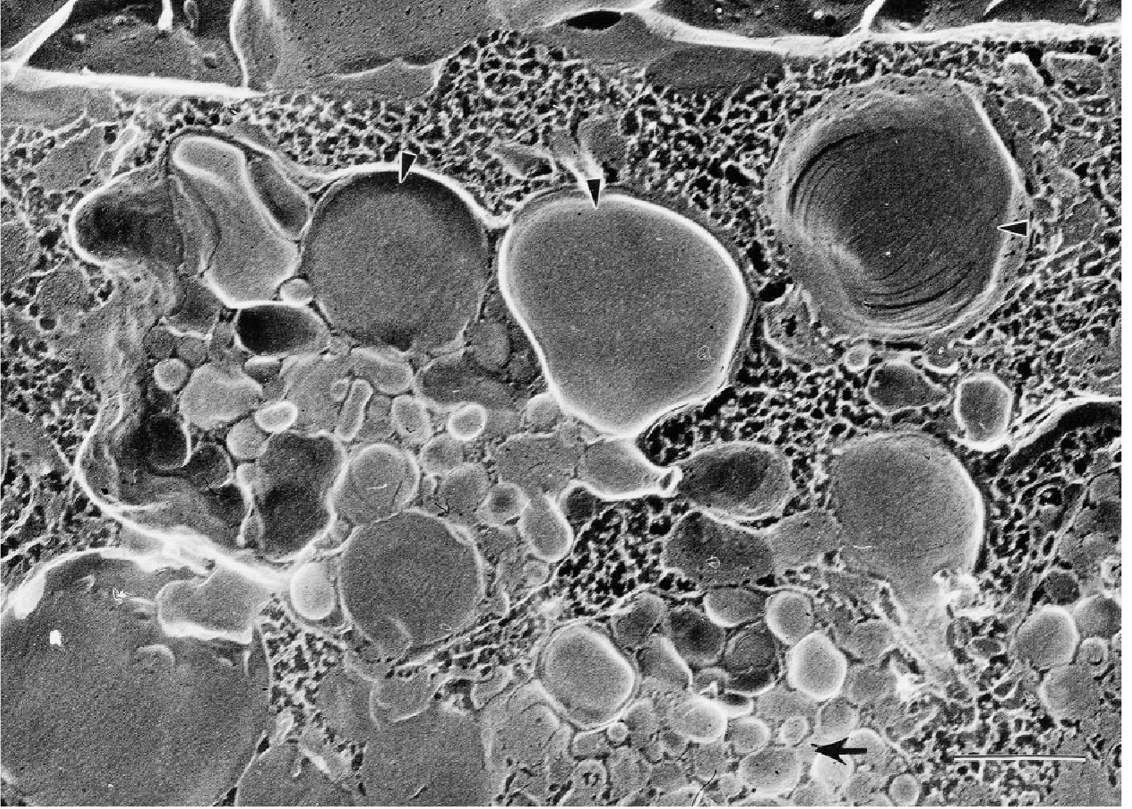
Cone electron microscopic Image : A macrophage after a diet full of LDL molecules
There are innumerable evidence for LDL, being the enemy number one in human atherosclerosis .It don’t know but, it fully deserve the name bad cholesterol.It looks like it may be counting its last few decades, as the whole pharma industry is activated to destroy this physiological molecule that carries some critical functions in our body. In one of the hyper-educated debate, I asked how low we can bring LDL down ? One leading professor of lipidology with a H index possibly crossing his LDL levels, said, we can go as low as possible , even to zero. He argued for possible eradication of this heinous molecule. No surprise, there was a thunderous applause from the industry benches.
How to go about lowering the LDL ?
Statins are the first line drugs. We have found it is not enough, it doesn’t bring down LDL below 70 in many , enhancing the residual risk .Now, we have found a God sent weapon. PCSK has got into our hands after some stunning collaborative research between geneticists, biochemist and pharma guys. Let us use it judiciously . This LDL receptor regulatory chaperone , prevents its recycling so blocking or reducing its function
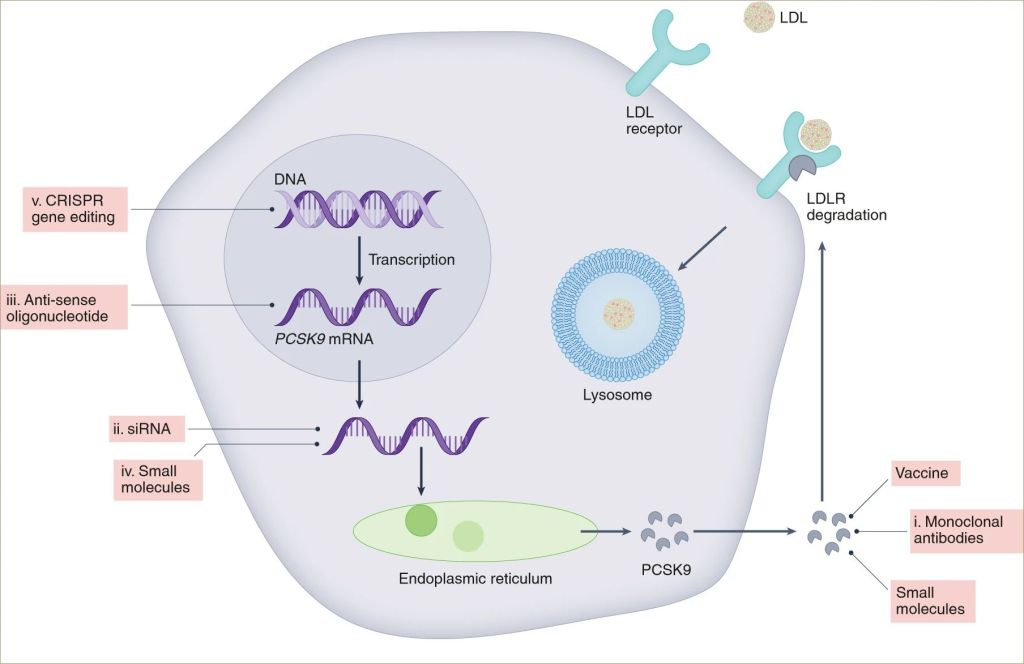
This cartoon from the Dr. Libby’s article (Ref. 1) image depicts the potential pathways beyond Evolocumab (Repatha) and Alirocumab (Praluent). PCSK can either be blocked after its synthesis or paralyzed before it is synthesized (RNA manipulation therapy SiRNA). There is one hidden face for PCSK trials as exposed by BMJ report of FOURIER methodology that will argue some caution with this new target.
Bembidoic acid is a also can also join the death game of LDL .It just acts two step above the HMG-CoA axis blocking ATP citrate lyase, . BM-Acid is approved by FDA well before the CLEAR trial by Steven E. Nissen et al NEJM 2023Leqvio ® (Inclisiran) is also approved in 2023. Soon, we will get vaccines that will promote lipid catabolism.
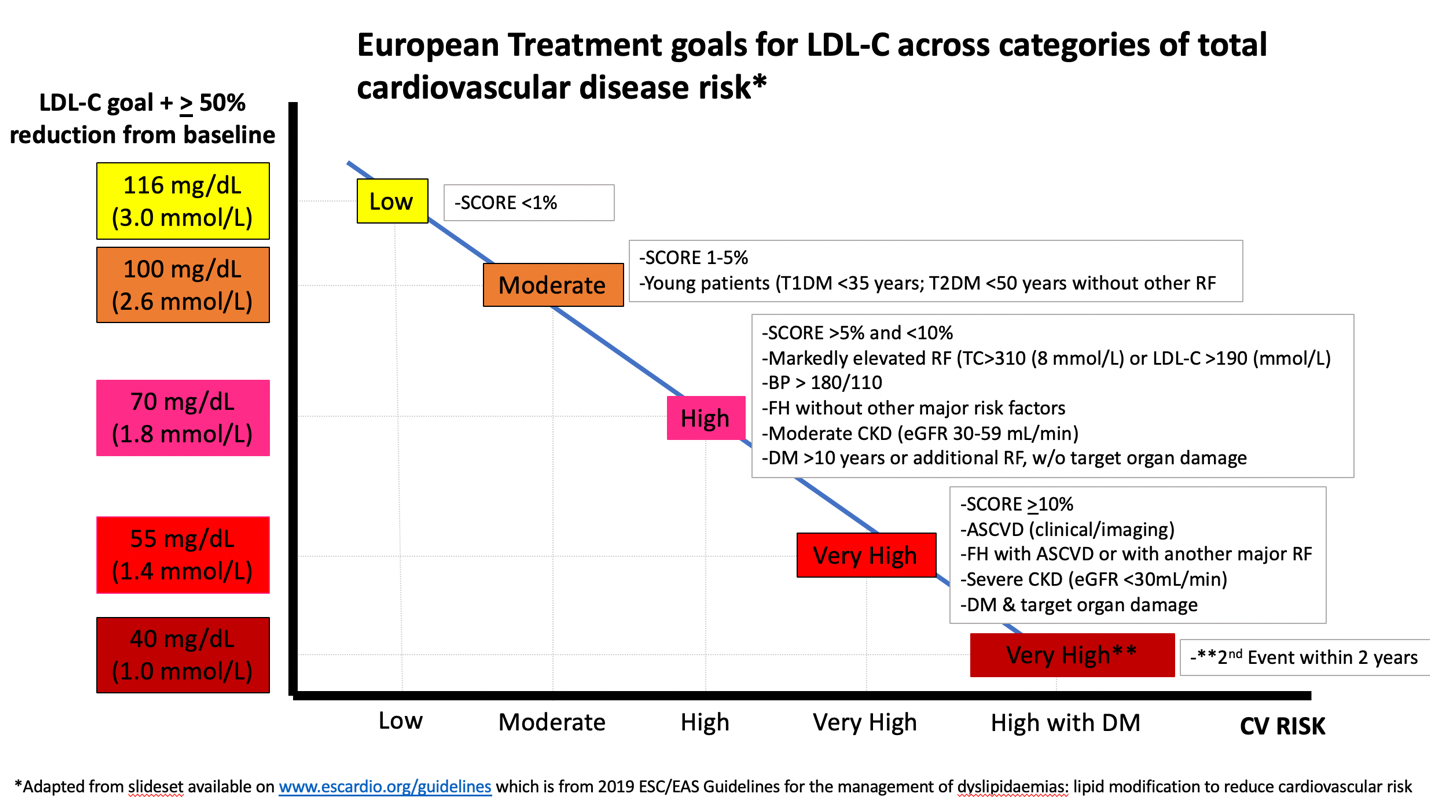
Ok let us be practical : What does the current guidelines say about LDL target?
It depends upon the risk profile and the guidelines you follow. Numbers to remember are 70, 55, 40 mg
One of my suggestion is to try keep both LDL and HDL as narrow as possible. This would mean both LDL &HDL should hover around 55-60mg in high risk category
Can we allow the proposed free fall of LDL ? (Ref 2)
If we apply the 50% reduction from baseline criteria, if someone develops CAD at 50 mg, it would mean to reduce LDL to 25 mg, right? This is where the problem starts. LDL, apart from being a carrier of hormones, may have a role in the structural stability of every cell membrane. While, the relationship between LDL and atherosclerosis is so intimate, funnily we have heaps of data that show South Asian population with tons & tons of plaque with normal LDL. The lesson we haven’t learned from the Indian paradox is that there are more unknown and invisible culprits in promoting atherosclerosis and CAD.
*In fact, for the future generations, there is more exciting ignorance waiting to be decoded. CAD without standard modifiable risk factor SMURF is the new agenda (nearly 25% of CAD occurs in the absence of SMURF – Ref -3). In this scenario, whipping a single known culprit and playing the LDL number game among the public mind is not welcome.
Final message
The tendency to portray a physiological molecule LDL , as a sole villain for CAD is not correct. Further ,trying to eradicate it, Implies, inadequate understanding of human lipidology.
It was 1823, a genesis of a new thought process in medical publication began. The man who started it all, Dr.Thomas Wakley the founder of the most famous medical journal (Ref 1)
One of his peers described him what sort of an Image he had. “Thomas Wakley the editor as we find him—a courageous challenger of the medical establishment who was usually right and whose language, however tasteless it might seem today, was well suited to the rough and tumble of the time in which he wrote and spoke”
Lancet celebrates 200 year anniversary
On this 200th anniversary Lancet , looks back ,introspects and redefine the agenda of medical profession. We need more and more people like Wakley in the current era.
The Lancet editorial team has come out with two clips one podcast and other a brief video for a total of 28 minutes . If you have enough patience to hear to this , you are probably in the right direction to understand what exactly is the purpose being a Doctor.
After going through the history of medicine through the lens of Lancet, and understanding its original motto, one thing is very clear. Science and research are vital for progression medical science . But, the least important enemy to handle for a healthy planet and mankind is not diseases and afflictions as such, but the unkind behaviour of biased power centres, skewed knowledge, and unhealthy & unequal practices of health care invention and delivery.
Final message
Doctors are primarily healers, all right; more importantly, they are guardians of goodness and justice in healthcare. For this, we need to “Wakleyse the medical education“, meaning, keep a watch always on the true aim and action of medical establishment under which you work . I know, this post might sound pessimistic for many of you, … but that’s where optimistic goals are hidden deep .
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.