Courtesy : A news clip from The Guardian , UK 26th December2024.
Can any one dare to stop this prescription medication with significant metabolic side effects ,being flashed in the New York bill board ?
Semaglutide is a GLP 1 agonist, (Glucagon like peptide) primarily used in diabetes where it competes with glucagon and modulates its adverse action. By some unknown mechanism this drug reduces body weight. The consequences of which is not clear. Meanwhile this drug got cleared as a magic bullet , as a weekly shot injection in obesity .We don’t yet know the long term effects of this drug. But, already it is promoted in social media, (as if it is a Pepsi or Coke) bypassing the physicians. It is a new low in pharma marketing strategies. (No one bothers, rather, no one wants to bother.)
Final message
The primary issue here is, not about the quick buck of profit, these companies want to make. It is about the potential Injury it can cause to patient’s ,(rather, healthy peoples’)metabolic landscape.
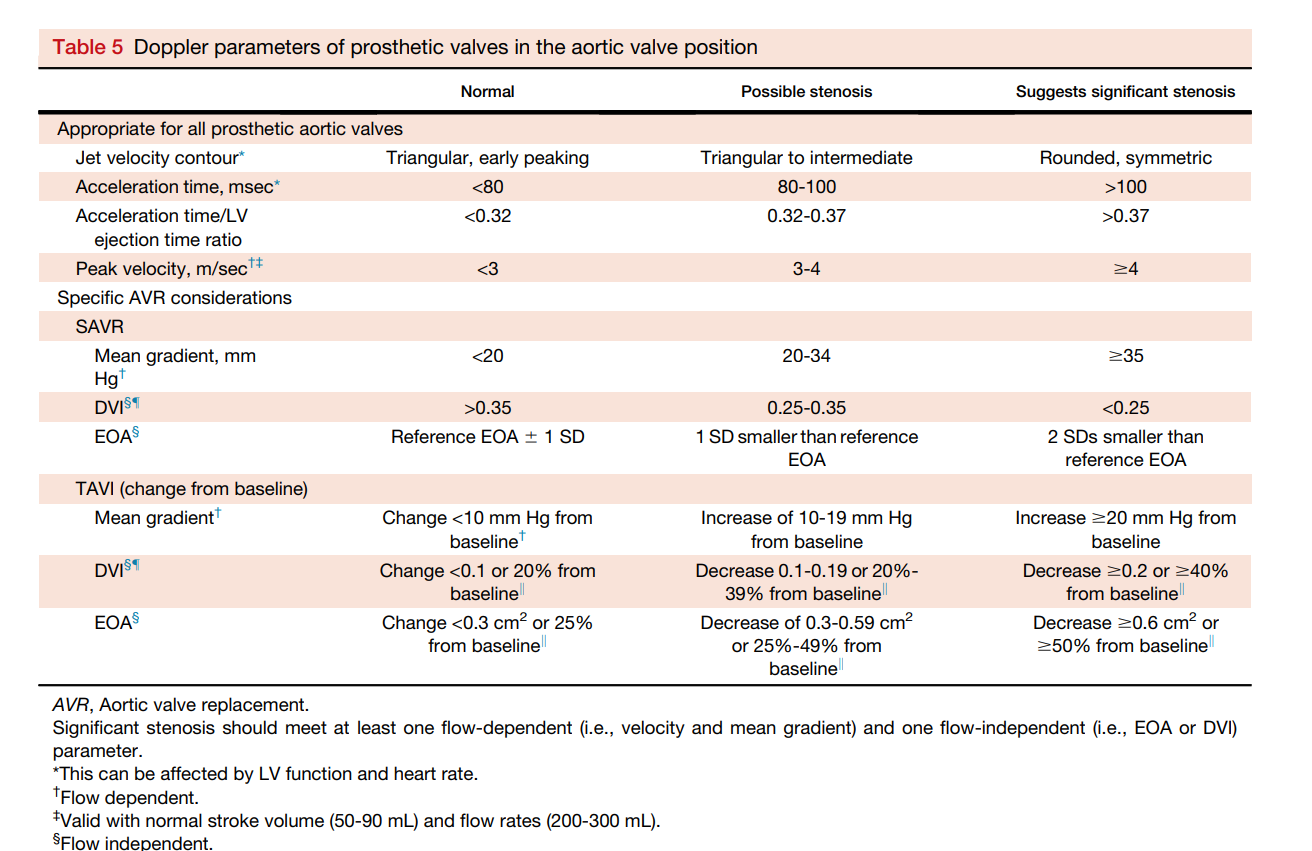
Prosthetic valve assessment is complex, thought process intensive examination. Not every echocardiographer can do it efficiently. It needs a good knowledge of anatomy, physiology of inter & Intra valvular hemodynamics .It demands thorough understanding of principles of Doppler echocardiography and also the hidden truths( ie, How we take liberty with the mighty Bernoulli equation for granted )
In spite of the number of imaging and doppler parameters we are able to gather ,still, we need to analyze them with reference to the clinical presentation. Mind you, even an innocuous episode of fever, associated dyspnea, and tachycardia can elevate the mitral gradient and sound a false alarm.
Depending solely on prosthetic valve gradients to diagnose obstruction is the biggest error we commit. We have seen this, even from elite hospitals. Echocardiography is not the final say, one may require cine fluoroscopy, CT scan or even PET (Infected peri prosthetic abscess) in appropriate situations.
Absolutely yes. The number of studies with such wrong aims is staggeringly higher than we could imagine. “Wrong aim” is probably not the right word to describe them. Rather, we can call them obsolete, duplicate, illogical, unproductive, intentionally fraudulent studies, or studies with a prefixed conclusion.
There is an estimate, that says 95% of papers in nearly 5,000 medical journals, is either junk or written for the sake of publication related to mandatory academic positions or promotions as a budding scholar or faculty. Science has to survive on the shoulders of those rare & genuine 5% souls.
Final message
What is the true “Aim for your study” , I want a very honest answer ?
Yes sir, I agree ,the primary aim is to publish my damn paper and get that promotion !
A related post
There was a brief post about this in the year 2008, 15 years ago. Is it still relevant? Find out for yourself.
Here is astate of the art review article on peripartum cardiomyopathy from NEJM that came out in Jan 2024. It is one of the comprehensive article on the topic. Everyone will relish, and would like to preserve it as well . Click on the image for the PDF of the article .Sharing here purely for the academic purpose with the courtesy and thanks to NEJM group.
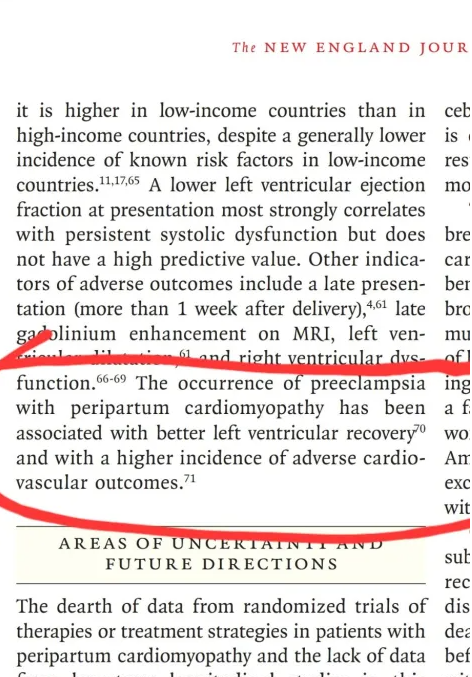
In this post, I wish to highlight two statements that occur in tandem in the latter half of the article‘ They are picked with one important academic purpose and a discussion on the combined entity of PIH associated PPCM.
I hope , you could appreciate the two lines (under the red bracket) to appear as antagonistic statements. Read the cross- references and try to understand yourself. They are not wrong statements for sure . It only reflects the complexity of the interaction of PIH with PPCM.
A 26 year old woman with PIH was about to deliver in one month, went on to develop another serious complication. Her echocardiography revealed LV dilatation with mild LV dysfunction. One reputed hospital labeled her as peripartum cardiomyopathy (flagged her as very high sub-set as well, since the PPCM has occurred in the antenatal period).
The family was in distress and blaming their fate. I happened to see her for a consult. It is true ,she fulfilled the criteria for PPCM with the available records. When I examined the patient, she was in class 2 and her BP was yet to be controlled fully. I added alpha methyl dopa for two weeks. I know it is just an afterload mismatch that has dilated her LV .Assured the family they need not panic, and she is going to have a good outcome if we control the BP tightly. The worried family was very much relieved and her husband wanted to know how I could give a good outcome when everyone was saying his wife was suffering from double complication.
Doctor, are you sure? My obstetrician says it is a deadly combination, but you ask us to take it casually.
No, I am not asking you to take it casually. It is indeed high-risk pregnancy, but the outcome is not as bad as we predict, especially in your wife’s case (A combo of PIH with PPCM ) where we have a target to treat .
As I expected (with all concealed anxiety) the mother delivered a normal baby with a little bit of lung congestion in the immediate postpartum period .However , she recovered fast , discharged doing fine in follow-up. LV shrunk back to normal dimension two weeks.
Is PIH and PPCM are pathophysiologically linked ?
Peripartum cardiomyopathy is a complex primary/secondary cardiomyopathy with varied outcomes. It is a neurovascular and hormonal disorder, affecting the heart and possibly the entire vascular system. It is important to note, this happens in a rare population of genetically predisposed individual, who harbor molecular defects in cardiac structural muscle proteins and gap junctions.
It shares some of its pathologies with PPCM and affects the placental, uterine, and microcirculatory vascular bed, impacting the perfusion of the growing fetus. In the process, it gives false autoregulatory signals to the mother’s circulation, which responds with a dramatic increase in late pregnancy trying to perfuse the baby , reflecting natural mother-baby evolutionary survival model. This includes the RASS system , and for this reason only ACEI are an absolute contraindication in pregnancy.
PPCM is a rare but not a mystery diagnosis,. Obstetricians out of anxiety and compulsion refer to cardiologists every case of pregnancy ,(of course in your case it is a must, since it is established PIH ) Further, the current echo machines are too sensitive to pick up mild abnormalities. It is very important patients should be relaxed during echo. If the resting BP is high, LV wall will be stressed, global hypokinesia can occur . Often times , we have wrongly labeled transient LV dysfunction due to sudden spikes in BP as serious cardiac muscle diseases. This concept is called afterload mismatch.
This process can have drastic effects on the mother’s heart, as the response to raised afterload is unpredictable. This disease affects the maternal circulation primarily by increasing the BP. What is the heart’s response to this ? It can be a fight mode with development of LVH or a flight (fear) mode, ie dilatation of LV that may end up in echocardiographic LV dysfunction or clinical failure. We are comfortable in labeling this as a type of PPCM. Many such mothers do well once the baby is out and when the BP is normalized.
.
Final message
PIH increases the incidence of PPCM in the general population. While the prevalence of PIH in PPCM is 22%, the incidence of PPCM in PIH is a far lower(.05 to 1%) The outcome of PPCM is often dismal (18-56% Ref JAMA 2000) with mean mortality reaching 30 to 40%.
Though PIH appear in the adverse list, what we find find in the real world is , PPCM that is associated (most likely triggered) by PIH/preeclampsia has a much more favorable prognosis than other mysterious /idiopathic forms of PPCM. However ,the degree of LV dysfunction determine the ultimate recovery ,even in PIH associated PPCM.
In this era of Artificial ignorance , using mathematical models for biological risk prediction can be tricky or even misleading .PIH and PPCM are two high risk subsets, when looked in isolation, but when they occur together, the risks actually need not add up. Infact, it is plausible , LV dilatation in severe PIH could be a marker of utilization of cardiac reserve mechanism, which has crossed its limits transiently.
A post amble paradox
PPCM, if it occurs in the antenatal period, obviously It is more risky, because the mother has to pass through the test of labor or cesarean with a dysfunctional heart. Ironically, most of the PIH-related PPCM is expected to occur in the antenatal period, which may ultimately carry a better outcome
Ventricular tachycardia can be a killer arrhythmia that can arrest the heart within seconds or behave like your pet, gently cuddling the heart and terminating spontaneously. The latter phenomenon we call it casually as benign non-sustained VT. Such VTs are more common in the out flows, fascicles or in HCMs. Most of us do not have time, to wonder why some of these blessed arrhythmias are not able to sustain.
Of course, the definition of non sustained VT can be challenging and keep changing with time. We have examples for both extremes , ie hemodynamically stable sustained VTs as well as unstable , but still, not sustained one.
Coming back to the mechanism behind these VT ,Let me provoke an answer from the readers.
Why some VTs are non sustained ?
A. The forward head of VT energy front is weak.
B. Source-Sink mismatch and tissue fatigue .
C.Disconnect between upper & lower loop of VT
D.Rate induced functional Exit or Entry block in the circuit
E. All of the above
F. None of the above , it is largely decided by the fate of the patient
While most EP specialists are busy taming the sustained one, very few are actively doing research about the mechanisms underlying the non-sustainability of VT. Here is interesting paper that discusses possible mechanism of termination of re-entrant VT.
The clinical importance of this question is, if we can convert sustained VT to non-sustained ones with drugs, it is indeed a therapeutic success. Drugs can slow down or terminate the arrhytmia circuit by acting in any of the four phases of action potential. The research in the field of anti-arrhythmic drugs has almost stopped in the last four decades for some unexplained reason. I think, we (Pharma companies?) decided to close the doors of anti-arrhythmic drugs after Dronedarone or Ibutilide . Renewed interest in Mexiletine, Norpace and Sotolol is a welcome move though. My suggestion is, oral forms of cardio specific lignocaine analogues could be a game changer in the filed of cardiac arrhythmias. Phenytoin sodium is old warrior drug, could make a comeback.
If only we had tried more, we might have produced more powerful drugs ( One obvious reason being cardiologists have decided to take on cardiac arrhythmias with electrical and mechanical weaponry in the hope of avoiding drugs. But, that aim has not really been accomplished except in AVNRT/AVRT. We still need the assistance of drugs in many classes of VT, even after ablation as well as an ICD.
Final message
As far as the answer to the MCQ, is concerned, response E is correct. If we look at the question again, quixotically, we may need to agree response F, (ie none of the above) is also right. Destiny decides the presence or absence of factors A to D in a given patient.
Fixing the target LDL, in both primary and secondary prevention is becoming more & more complex . The reason being, there is a huge healthy population ( with zero risk factor) , but showing insignificant or minimal coronary plaques. This subset of population is anxiously unmasked by inclusion of CT angiogram in many master health check-up programs.
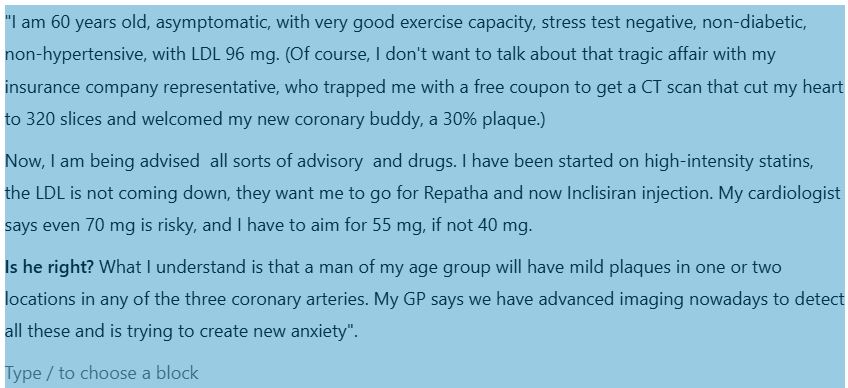
A case profile& a debate
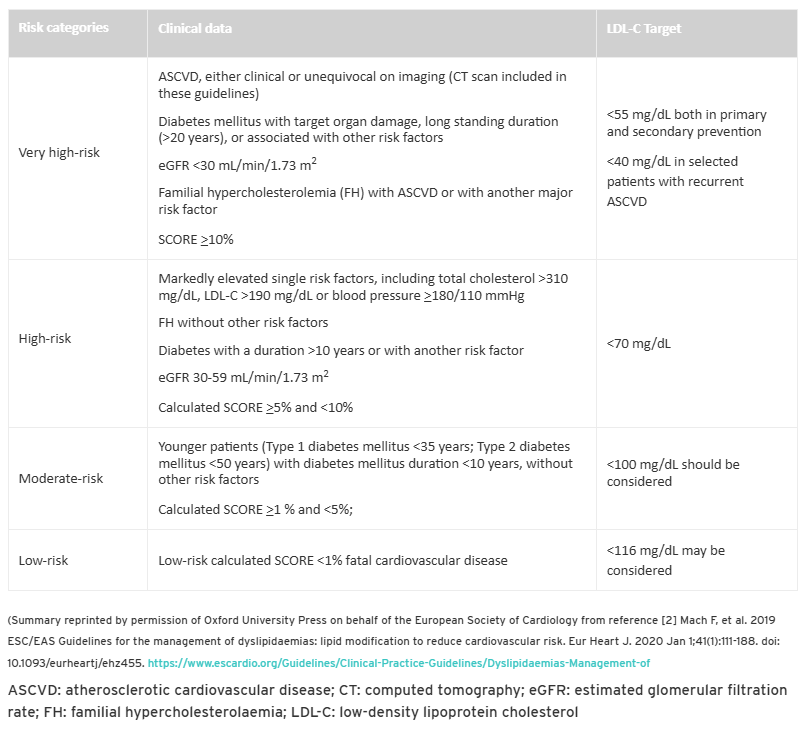
What does the guidelines say ?
If you have any athero-sclerotic cardio vascular disease(ASVD) documented by clinical or Imaging , you belong to very high risk category. It clearly says the target is 55mg both in primary and secondary prevention.
LDL is not only the enemy of the coronary artery. Fatty streaks in the coronary artery begin in the fetal stage itself. In adults, some of these streaks become prominent locally and turn out to be plaque. The argument for intensive statin therapy is to stabilize these plaques. We would not know if the plaque is stable or not. We can’t do OCT imaging, an invasive test, to know about the vulnerability. So, for the sake of safety, everyone advises intense statin therapy. The irony is ACS continues to occur at any level of LDL.
Final message
Is my cardiologist right about the LDL target of 55 mg ?
If you look at the above table of risk categorization, your cardiologist may be right. But the deeper issue is whether such a recommendation is correct or not. In our opinion LDL 70mg is good target to achieve. Lowering further, has its own risk. I am sorry, you can’t escape from the guidelines as of now, Further you don’t have any other risk factors to treat as well. Then, this question, will always hang above your shoulders , why the hell I got this plaque over there?
I think ,its time ,we need ask more questions that are difficult to answer ?
1.Does ASVD includes even 10-20 % plaques by CT angiogram ? How specific these X RAY – stitched slices of CT scans done on moving heart. Then ,what about luminal irregularities ? Should it to be counted as ASCVD as well ?
2.Do we need to refine the definition of by introducing a new term significant ASCVD?
3.Also like subcategorization of clinical ASCVD from image-based ASCVD with reference to target LDL?
Dear patient, wait, there can be more shocking advisories soon. With the famous PREVENT trial (Lancet 2024), results are waiting on the sidelines trying to penetrate the fragile barriers of various guideline writing committee offices. By the way, PREVENT study demands an OCT for all non-flow limiting plaques, and stents if they are found be vulnerable.( Read about The TCFA story)
We keep doing RCT after RCT trying to find out the truth, whether opening CTOs are really useful. Meanwhile, cardiologists continue to do CTO- PCI as per their wishes, convenience, and perception of the literature.
5 major studies are available about the utility of PCI in CTO
It seems, it is far easier to do multiple, multicenter RCTs than to interpret the findings of these trial results. However , we have mastered the art of tunnelling down blindly, both in the ante & retro grade routes , tackling the tortuous and often rocky, CTO terrains and complete a wonderful PCI. Still, we are not sure ,whether it is worth all the efforts and risk ?
What does it mean? It conveys a simple truth. Our hands work more brilliantly than the brains.
Of the above four, only the DECSION -CTO was negative, still many cardiologists are not ok to do a CTO PCI . Why ? The reason is simple. They know the truth that, none of trials showed improvement in overall survival .
Most studies looked only at angina as a symptom .Very few included patients with dyspnea as a symptom . While it is rare to recruit asymptomatic patients in clinical trials, in real world it do happen very often, ie getting rid of the block as an indication .
We do get some useful information from these trials
1.Expertise and hardware .We have good technology to do a successful PCI .
2.Don’t open it just because you do it
3..Simple documentation of viability is not enough. We have top prove the same viable segment is critically ischemic as well .The buck doesn’t stop there, the procedure we do should be good enough to eliminate that ischemia ,
4.If symptoms are angina and it is refractory, one may consider CTO PCI. Never do it for relief of dyspnea, even if the guidelines suggest you to do so.
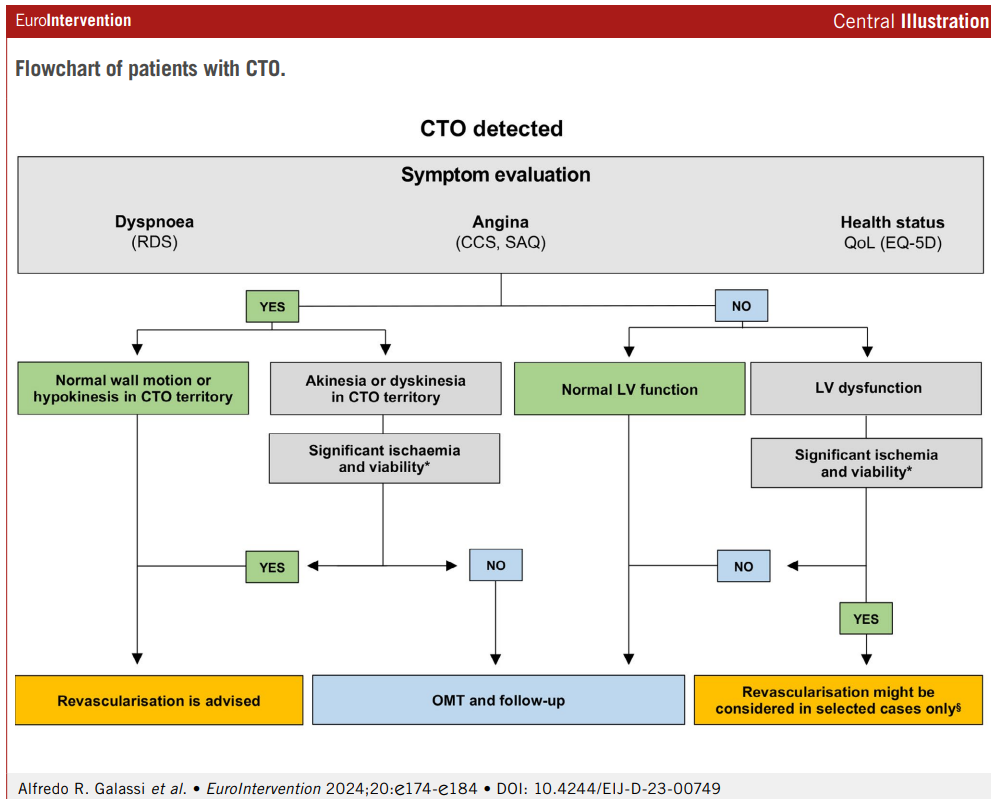
When can do a PCI in CTO without guilt ?
We do have official algorithm
CTO procedure deftly improves both cardiologist’s’ & patient’s sense of well-being, provided the patient doesn’t experience any complications, which can be anything between 3 to 20%.
Why Indication for CTO PCI are still tentative and vague ?
*We are yet to do a proper study addressing all the important variables in the CTO pathology and hemodynamics.
*Even if, we do a good study , they are not properly interpreted.
*Even if it is properly interpreted, guideline writing committees tend to be biased towards more action than inaction.
*It is strange ,Inaction (not doing a PCI) is seen as a therapeutic defeat for a cardiologist as he leaves a patient, who has a blocked coronary artery, however healthy he may be.
Conclusion
If we are not able to arrive at a meaningful conclusion even after many RCTs on the on the same topic ,what does it mean?
It could mean only one thing. Studies and trials are not the real answer to the questions which we are asking .There is something more we have to look at. Mathematics and biology can’t be fused as we desire.
The following thought, is in response to a spate of violent attacks by patients on the doctors in my state. One of my ex-colleagues, an Oncologist was stabbed with a knife by a son of an elderly mother in his clinic room, apparently agitated with the side effects of the chemotherapeutic drugs she was receiving for end-stage Hodgkin’s lymphoma. The other case was a young gynecologist attacked for the loss of a newborn baby due to obstructed labor, again alleging wrong care.
A chilling concern and a confession
While doctors work day in and day out for the welfare of the patients, it is inevitable that forces beyond their control and some systemic issues do bring some adverse impact. Critical decisions are taken on a moment to moment basis, guided by their experience ,Intuition, trust, and belief, of course with learned skill and expertise. It is estimated that doctors work with a knowledge base calculated at best 20 % for most illnesses. ( BMJ 2022;376:o702) So, we primarily work with what we don’t know, rather than what we know. Unfortunately, no doctor would like to tell this, and no patient wants to hear this. But one thing is certain. No doctor can ever harm a patient intentionally, even in dreams.
However, errors in judgment and negligence, along with some casualness due to physical and mental stress, do happen. To be honest, it is more common than anyone can guess. Fortunately, the bulk of these errors are not reported and either self-heal or are rectified internally without reporting. I can also say with conviction that doctors are humble souls, and most of them carry the guilt of a true error lifelong and take every step to prevent it from recurring. (Recalling the tragic story of an honest gynecologist Dr Archana sharma who committed suicide due to mob shaming)
Minimizing such harm is one of the major goal of every doctor and institutions. However, it can not be eliminated completely at any state of imagination.(It is like climate change in environment or corruption in politics) To repeat this statement ,No doctors can harm a patient intentionally, complications, and errors are like high way accidents .Request the patients to please understand this simple truth. Many patients do, many don’t.
The problem with many patients are ,they are unaware, that doctors often practice medicine with incomplete knowledge. To be very frank, many times it turns out to be , sort of therapeutic experiment with inherent risk at every stage .The present day patients want to know ,what the doctors themselves do not know.
There is new emerging issue. the current generation of patients in our part of the world ,carry a huge and unrealistic expectation along with lowest level of tolerance. Armed with artificial ignorance fed by digital doctors ,they think if you have money power, we can cure any disease. . It has gone to the extent , they are not able to accept even the natural history of untreatable and end-stage diseases. Some of them harbor a dangerous thought ,that no patient dies in a hospital instead ,he gets killed by mis-management.
“One of the important reasons for this miscommunication, squarely lies with us. We need to admit, un-intentional errors is indeed a big problem in medical profession, as in any other field”
Final message
Even serious errors in other public departments like transport, economics , Judiciary , police ( even intentional criminal acts by individuals ) are casually taken by the public and readily forgotten or forgiven. While ,the tragic truth in our profession is, patients are never ready to forgive even small errors by doctors who have dedicated their entire life for patient welfare. Unless something dramatically happen that change people’s perception about medical profession ,we are heading towards very tough times.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.