For right or wrong reasons, the world of electrophysiology has pushed us into a belief system that, if it is AF, the culprit must be pulmonary veins. In fact, non-pulmonary vein origins can be a staggering 70% in some series. (See below) It can be in the free walls of the left atrium, LA appendage, IAS, IV, SVC junctions, coronary sinus, ligament of Marshall, crista terminalis, etc. (Ref 2)
For example , where will be the initial focal trigger for AF in a pateint with COPD ?
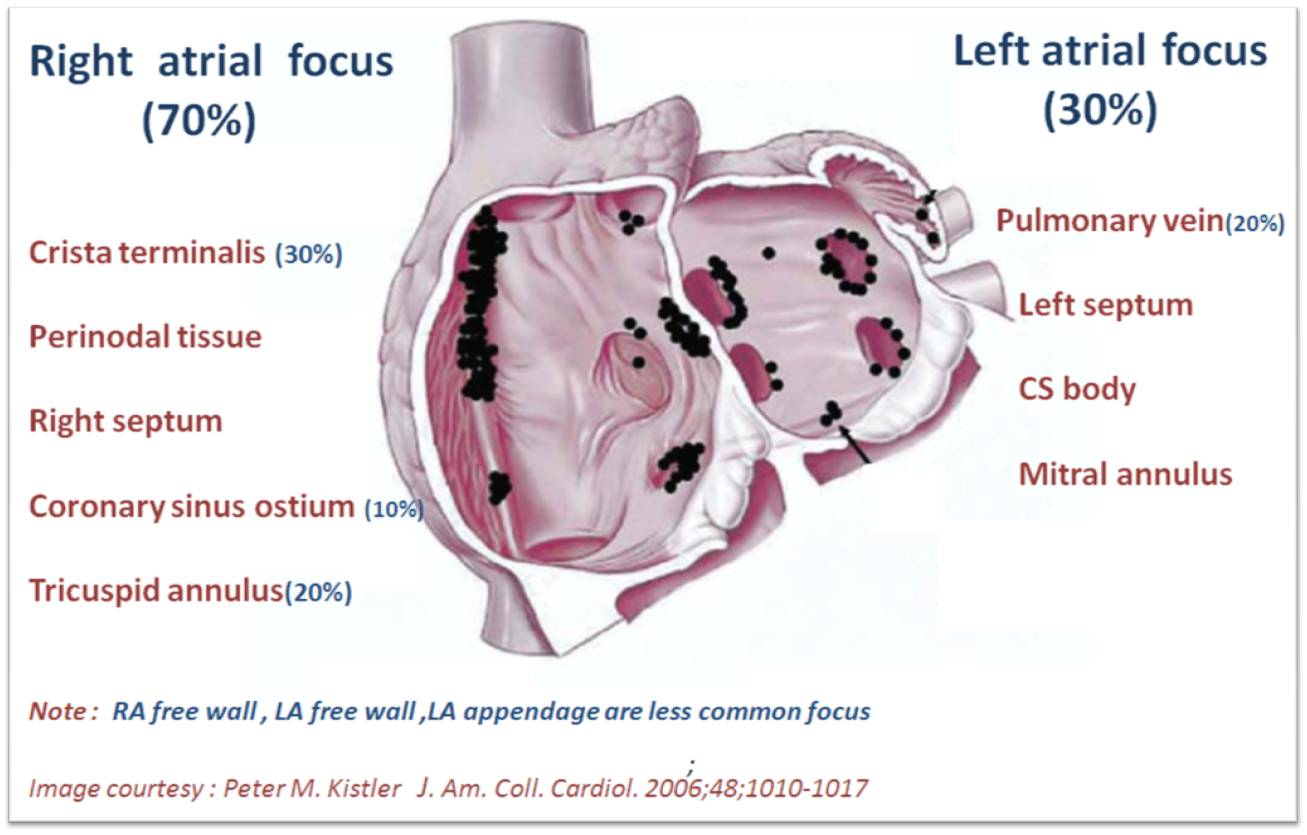
Can you ever think of ablating PVs in a patient with AF and COPD, where the right atrium is under stress and strain? It doesn’t require any extraordinary intelligence to conclude any chronic focal atrial tachycardia can get degenerated to AF in the long run. In that case, the famous atrial tachycardia localizing map from Peter Kistler et al from Australia JACC 2006 holds good for location AF focus too.
If we look at the above map,RA prevails over LA convincigly in termes of focal atrial tachycardia. Only 20% of focal AT arise from pulmonary veins. I guess, the same should be true for AF.
Focus-less Atrial fibrillation
Right from the days of James Mckenzie, when AF was refered to as delirium cordis or ataxia of pulse, AF was always considered as a chaotic, focus-less arrhythmia. It is still true in many cases. The recent pulmonary vein triggers are just a small revelation and need not be a revolutionary paradigm shift , as we are taught. There are innumerable patients who develop de-novo AF without any focus. Hypoxic or acidotic milleu of a single atrial myocyte can iniitiate an AF, alosan episode of atrial ischemia, diffuse inflammation as in atrial epi-myocardiits can trigger AF from any spot on the atrium.
As India celebrates its 75th Republic day anniversary, we hear a silent news, of loss of its one of the great citizens , a doctor , a scientist and humanist par excellence. DrKotturathu Mammen Cherian
Wars and scientific debates do not end that easily. Parallel to the Vietnam war days of 1970s to the current Ukraine-Russia conflict of 2025, one silent academic war is going on, in the conflict-ridden corridors of cardiology and cardiac surgery. (The CASS study of 1970s to the ORBITA era of 2025) Any amount of scientific literature, debates, guidelines, failed to tick the right choice of revascularisation in chronic CAD. Ironically, as our knowledge increased the decision making process got more murky.(Largely due to non academic factors)
To find an answer to this, CTSNET, a hugely popular cardiac surgery forum orgainsed a seminar trying to create a globally unifying approach. This is an hour long seminar , I am sure will enlighten us further. Please make yourself free for 60 minutes. Better , not to go to the summary, without watching the video.
1.First and foremost, academic guidelines are created primarily, to make us understand the disease process fully, which would help us make a good decision. Interpretation of these guidelines can vary widely . As a professional physician , we are supposed to use the official guidlines judiously, at no time, we can be slaves to them.
2. It is possible ,the term myocardial revascularisation itself is largely misunderstood. What is being vascularised ? & What is the impact of that vascularisation are the right questions to be asked.I feel this seminar genuinely adds some sense to the flawed understanding of the prevailing concept of myocardial revascularization.
3.Think mechanistically and extrapolate the potential benefits and risks .Try to sort out the issue individually. Recall the classic truth that, revascularisation rarely improve contractility in chronic LV dysfunction to the desired levels.(Inspite of the patchy benefits shown by CABG-PATCH/ REVIVED BCIS-2 trials)
4. Realise, the confusion in choice of revascularisation is more in chronic coronary syndromes. PCI has an edge in acute situations if done in a timely fashion.
5. It is a open secret ,there is a big conflict of interest in the guideline writing committee. A huge transatlantic academic gap exists with American guidelines of 2021, 2023 favoring more PCI, while ESC recommends more CABG in complex lesions and left main. The big controversy ,that brewed was when Indication 2A was confered for both PCI and CABG in left main and multivessel CAD.
6.Global experts unanimously endoresed the European guidelines ,which favors for more liberal CABG . Still, they were hesitant to denounce the American guildelines.
7. Curiously, I believe the debate question itself is not fair.We should not be debating PCI vs. CABG at all ? This makes GDMT not a standalone option at all. In both hindsight and foresight, this may be the best option in the majority of patients, as indicated by many landmark studies of revascularization.(There is an Interesting comment made by the panelist relevant to the above point)
8.Every CAD patient should have an option finalising his decision with a heart team comprising of a clinical cardiologist, an Interventional cardiologist and the cardiac surgeon .
9.Quality and expertise of surgeons and PCI team is vitally important.We can’t bring the same trial outcomes in any neigbourhood hospitals, especailly in less well developed countries.
10. Finally, most importantly, it is agreed by more experts that CABG has more potential to prevent a future MI than PCI in most subsets of patients. This is because, CABG gives realtive immunity to potential the disease progression in the proximal segments which are the original high risk zones .
Final message
I have shared some key personal observations triggered by this extrodinary seminar. It can be called as a personlised version and a summary .Please listen to it completely and try to find whether these observations are good enough.
ACS is one of the sinister diagnoses made at medical ER. The fear comes built in with the diagnosis often amplified by young felllows on call (& often times by senior consultants as well) It may appear real, from a clinical angle, but, please trust, when we deal with the whole gamut of ACS scenerios (other than STEMI), there is indeed a benign face, in many of them.
One big chunk of ACS-UA is secondary UA, where there is increased demand as in stable angina with tachycardia* . In these patients there is no plaque triggered ACS. For example, in a febrile patient who has associated HT, anemia, etc., we can witness menacingly deep resting ST depression with absolutely no thrombotic process going on in the coronary. (*Mind you, all stress-induced ST depression,, are not ACS, but a marker of chronic CAD.) I used to tell my fellows, a patient with hidden CAD, who develops fever for whatever reason, is acutually doing a tread mill test equivalent , and showing off the diagnosis. It is near- foolishness, if we rush them to cath lab.
How can biomarkers help us grade these ACSs?
The high sensitivity troponins not only help us to diagnose NSTEMI, it also tells us which one of them may be innocuous ACS or benign ? Strangely, we are also taught , “No ACS should be considered benign, until you see the coronary anatomy”. I wish patients realise, how difficult it is to practice cardiology, for that matter any field of emergency medicine. You can’t err at the same time , you are not supposed to treat inappropriate as well.
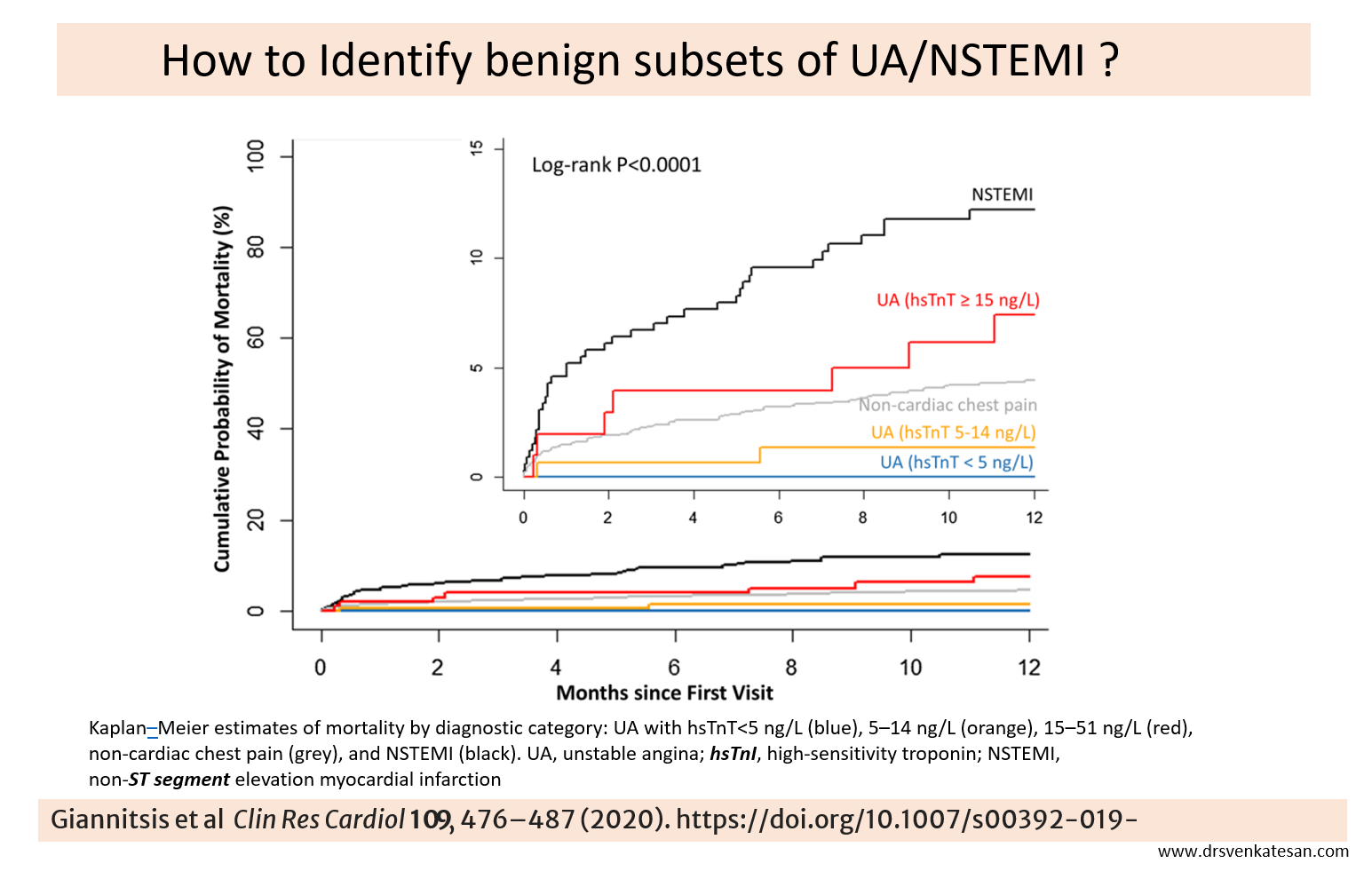
High sensitivity Troponin (hsTnT) do play a useful role in identifying low risk UA/NSTEMI , as seen in the following study. See how the Kaplans diverge dramatically depending upon the hsTnT levels. I don’t understand how the curve of non-cardiac chest pain trespasses in the middle of a Troponin race (False positives? Real concern then)
Final message
Clinical, biochemical, and overall risk profile assessments do help us risk stratify ACS. We have numerous predicting algorithms and scoring systems in UA/NSTEM led by GRACE, etc. Still, it can be a tricky game to make a call on ACS. Mind you, even a coronary angiogram will not bail you out in terms of decision-making and risk prediction. An incidental 80-90% lesion with a normal FFR is quite common.
Avoiding innocuous ACS patients getting admitted in CCUs is a real problem. Of course, getting trapped in a CCU for a few days is better than tampering with the coronaries in the cath lab. Some of the stakeholders may welcome both, but that is not science.
I recall some old guidelines saying not all UA need to be admitted. Many low-risk categories can be managed as outpatients; it is still true. I am not sure how many of us have the courage to do it. Courage alone is not sufficient; the fear of statistical misbehavior of ACS, compounded by potential ridicule from peers or even patients, always haunts.
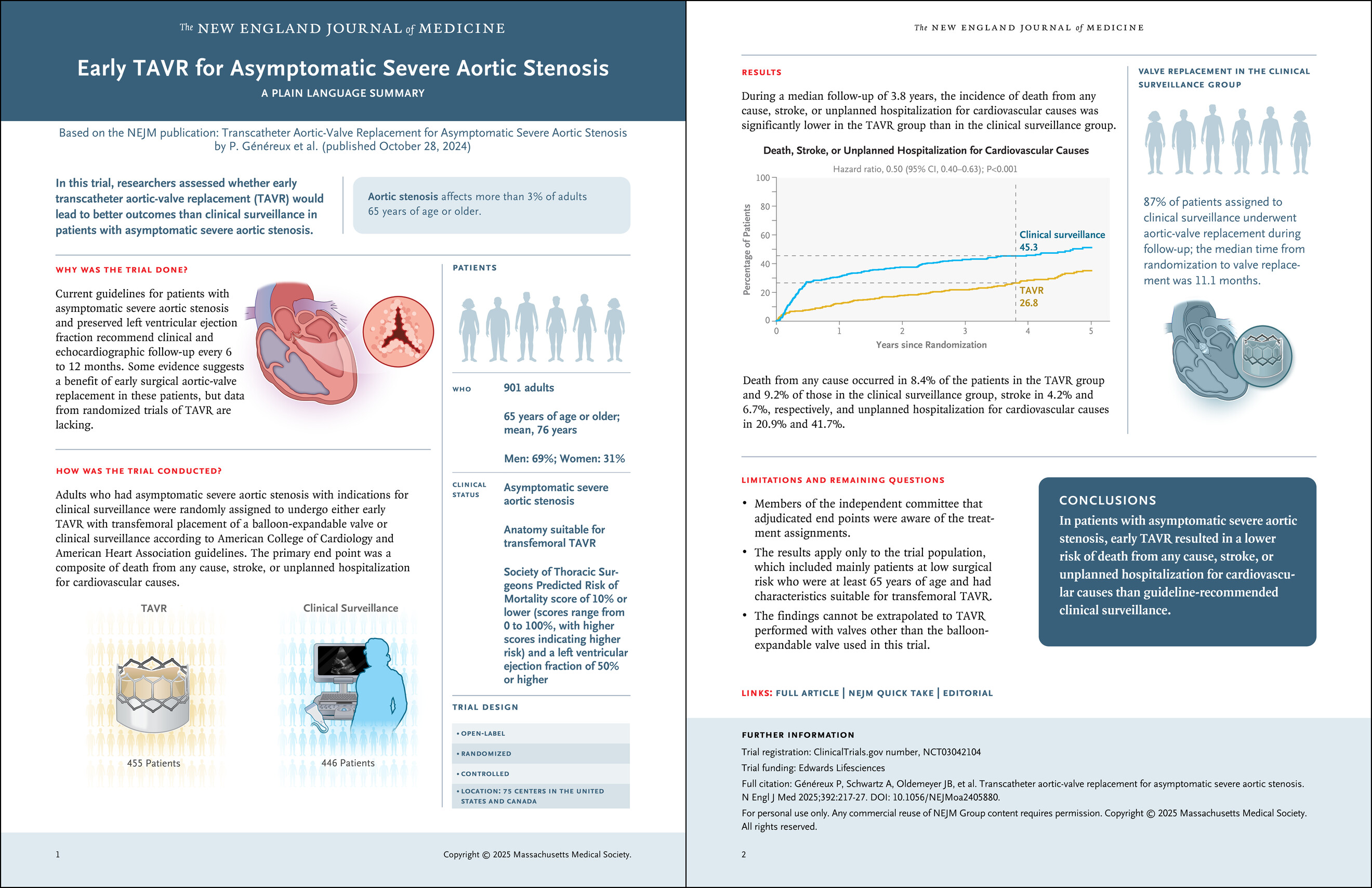
We know TAVI is in the striking distance , to literally take over most aortic valve interventions. From a humble beginning from very high surgical risk with prohibitive comorbidity, now it has almost touched the totally asymptomatic, relatively morbid-free patients. Thanks to the hardware, expertise, and motivation from multiple forces.
While the numbers increase, still the debate between SAVR and TAVR is riddled with speculation, skepticism, and absolute confidence. (Reason: TAVI is a passively fixed valve in a blind procedure at a self-selected annular plane, with no option to remove the crushed native leaflet debris and the resultant complications. Lastly, TAVI’s lifespan* is currently less than half of a mechanical valve. *Expected to improve with polymer valves)
The latest trial to join the litereture is EARLY TAVR in October 2024
Here is a brief, personal comment about the paper for non-academic consumption. Look carefully at the 15th second of the video. Pause it, look at the number over there on the bar of unplanned hospitalisation.
It is a staggering 41.7% in clinical surveillance group, twice more than TAVI group, pathologically tilting the conclusion of the study.
By the way, what is that unplanned hospital admission? Who is planning that admission in the asymptomatic control group? If 41% of people in the clinical surveillance group needed hospital admission, what does it mean? Does that mean clinical surveillance was so poor that they were rushed to the hospital despite being asymptomatic and stable in the surveillance period?
Why should totally asymptomatic patients get admitted in the control arm, in such huge numbers? You can presume what could be the reason. My guess is too sinister.
Another issue plaguing the RCTs for decades, is continuing even in 2025. That is putting together death, stroke, and unplanned hospital admission as a combined endpoint in the same basket. This is the familiar old cheat story i.e., used to intentionally torture the truth.
Final message
Any student with basic sense of statisitcs can interpret the result of this landmark trial from NEJM correctly. The question we need to ask is, what are the triggers for those unplanned hospital admissions?
Further, it is good for NEJM (and the medical community) not to accept any papers, if the studys’ endpoints are not appropriate or defined with the intention to manipulate, which happens in many sponsored trials.
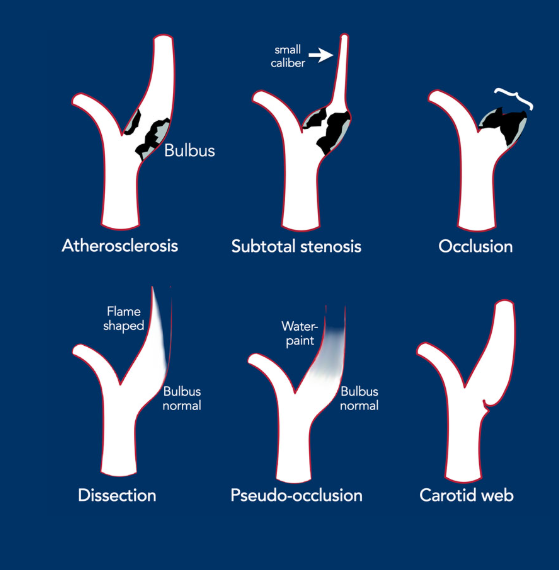
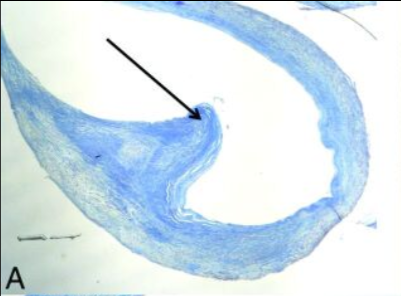
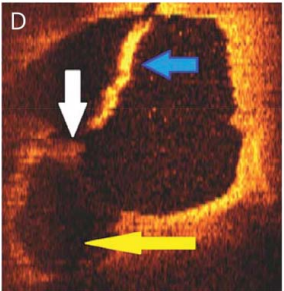
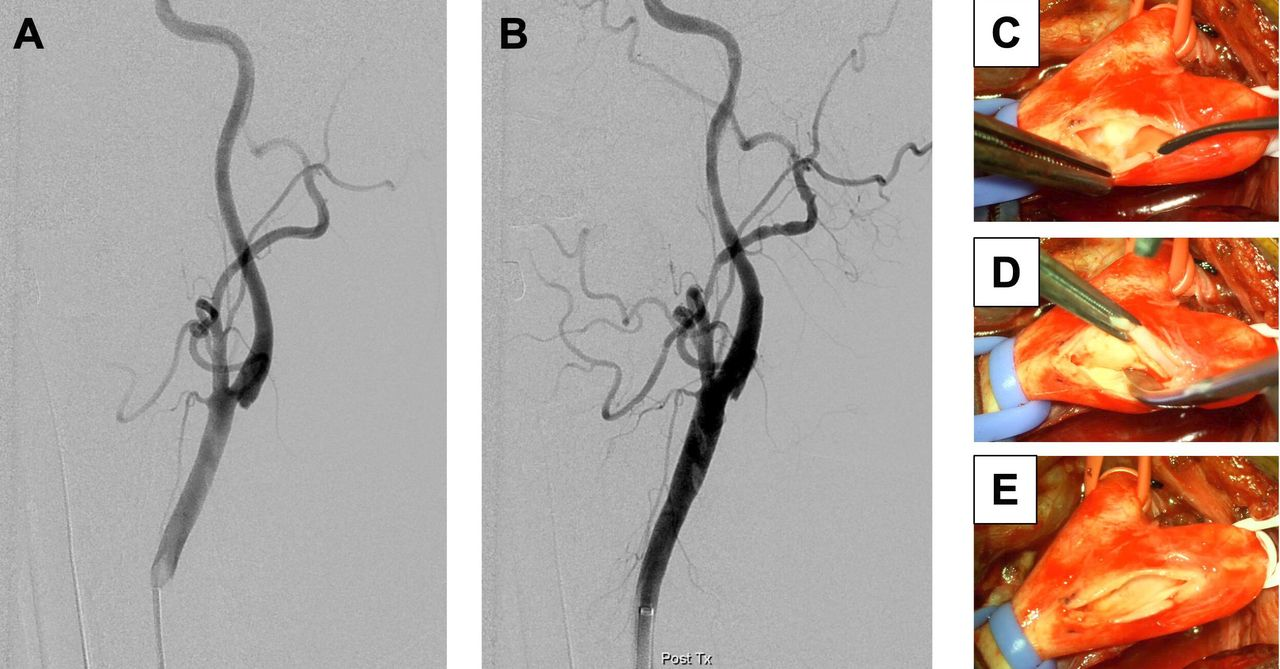
A carotid web is a shelf-like lesion along the posterior wall of the internal carotid artery bulb and an under-recognized cause of stroke in young individuals. Many studies suggest that patients with a carotid web have a high risk of recurrent stroke.
In the famous Dutch study on ischemic stroke MR CLEAN, 30 patients had carotid web which is around 2% incidence. In this study 1 out of every 6 patients with a symptomatic carotid web had a recurrent stroke within 2 years, suggesting that medical management alone may not provide sufficient protection for patients with a carotid web.
The web can create a flow disturbance, potentiating local thrombus formation, which can embolize producing resulting in cerebral ischemia. Current treatment is with anti-thrombotics and/or anticoagulation .Lesser option is to alter the flow disturbance caused by the web (surgery or stent).
Final message
Cartoid web is no longer a diagnostic curiosity. Its worth looking forit an any young patients with cryptogenic stroke.
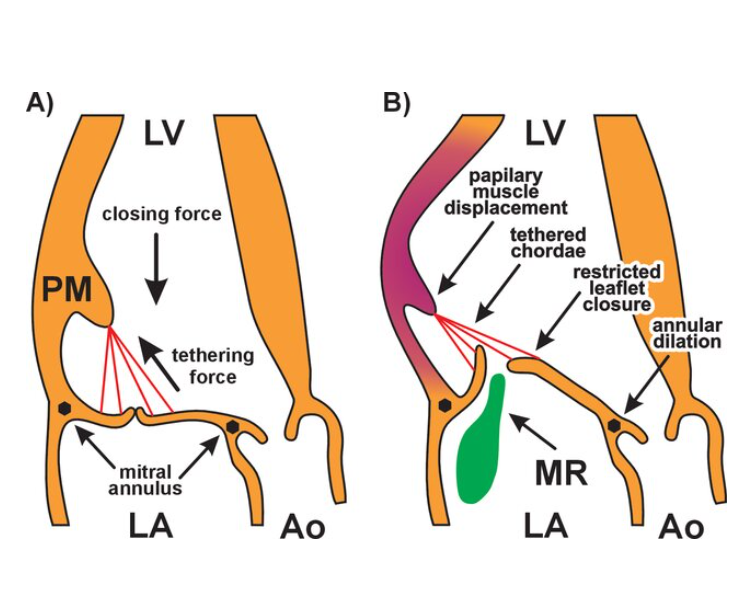
Functional MR is a term used , when it occurs due to defective LV function, ie LV dysfunction. This happens in spite of normal mitral leaflets and intrinsically normal mitral valve apparatus. The above statement can be instantly disputed because LV muscle is also a part of the apparatus. Then realistically, functional MR occurs due to dysfunctional LV and infact becomes a part of primary. Then, logically we need to replace the term functional MR to dysfunctional MR .A classical double oxymoron isn’t.
Image source : Barbara Brzezińska and Krystyna Łoboz-Grudzień from the Book : Structural Insufficiency Anomalies in Cardiac Valves Mechanism of functional mitral regurgitation. (A) Balance of closing and tethering forces acting on mitral leaflets during systole. (B) Disrupted balance of closing and tethering forces due to local LV remodeling (dark shading). LA: left atrium; LV: left ventricle; PM: papillary muscle; Ao: aorta; ME: mitral regurgitation.
Why fight with nomenclature ?
Classification and nomeclature are the foundation for any medical entity .Since, we build our knowledge over it, If it goes wrong, everything grows out of it is problamatic. This is exactly, is the reason we are blinking at the diagonally opposite results with COAPT & MITRA-FRtrials. Ofcourse , it is not a pleasnt job to shake the foundation often as well,as it has its own side effects.
It is expected in cardiology academic forums, we use the term secondary MR. While secondary MR is preferable, I guess myocardial MR may be a more apt term. We know secondary MR is further subdivided into ischemic and non-ischemic.
Need for a combined New entity : Combined Primary and Secondary(cps-MR)
This occurs in two situations
MR begets MR: If primary MR is severe, it invokes LV dilatation and dysfunction of LV . Then it becomes cps-MR by default.
Ischemic MR causing structural damage to chordae: If Ischemic MR ends up in chordal disruption or severe destruction of papillary muscle , it doubles up as combined primary & secondary MR
Final message
What is “functional” in functional MR ?
Nothing.Everything is dysfunctional. The only good thing is that the leaflets are structurally normal. (Please note, any of the other 5 components of MV may still be abnormal) Semantics and nomenclature should not bother us, as long as we understand the mechanism of MR and the principles of its management. Understanding the concept of cps-MR could throw more light on why the intermediate and long term outcome of MVR can be as unpredictable as a tropical storm in nay given case of secondary MR.
Postamble : If LV is part of mitral valve apparatus, then, let us realise the same thing will apply for RV as well. This would imply, right ventricle is a component of tricuspid valve apparatus .(at least to a lesser extent) This fact, is rarely taught to cardiology fellows.There is evidence for progresssive RV dysfunction, to worsen the TR, inspite of the reduced contractlity .The fact,TR begets TR, is less popular among us for no obvious reasom (Rana BS et al Echo Res Pract. 2019 )
Welcome to 2025 and best wishes for a great academic journey to all readers .
Collected from ACC website (Arranged in three heading) These are the creamy academic extract of whatever happened over the last one year. Thanks to ACC for compiling it. While the first one,(Trials) will be under scrutiny, the other two , ie the cardiology news stories and magazine reviews are absolute gem of learning resource.
What happened to top 10 cardiology research papers of 2023 ?Did we follow up ? what is the Impact of them in the bed side ?
For some reason, we have a strong belief , that randomized control trials (RCT) are the only way science can express itself and move forward . This is a much more sacred rule in cardiology. In that sense, every year, we see more than 100s of RCT get released various research centers with varying credibility. If every RCT is taken at its face value, we should have conquered much of cardiology secrets long ago. Unfortunately, that can not be the case.
As an Intelligent, interventional cardiologists we are extremely talented (From tackling a left main dissection, to recapture a runaway TAVI and reimplant it ) .But, we have to admit, many (?most) of us lack the expertise of picking the genuine , winning research especially in the arena of new drugs and devices. Some times, I wonder, whether we have sort of outsourced the job of interpreting the results to invisible third parties. No escape from this ,this is the way science has to grow.
Final message : One study from 2024 really bothers
The PREVENT trial of 2024 is suggesting a tectonic shift in the way we should manage CAD. It is asking for stenting all non-flow limiting lesion , if found, to carry high risk plaques by intracoronary Imaging. We have a come full circle, from vulnerable plaque to vulnerable patient and let us hope, we do not become a vulnerable cardiologist.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.






{kind=link}