Lifestyle modifications and non-pharmacological modalities should be started in every hypertensive individual before starting them on long-term drugs. This is one of the foundational lessons in the therapy of hypertension. (Please mind, in no way, it conveys a meaning that we can give less importance to them after starting drugs.)
Exercise prescription has become a big-ticket event in hypertension clinics in recent times. Though any physical activity in adequate quantity is good, we have classified exercise into complex subtypes and found fancy ways of its administration.
Traditional belief gets a kick-back
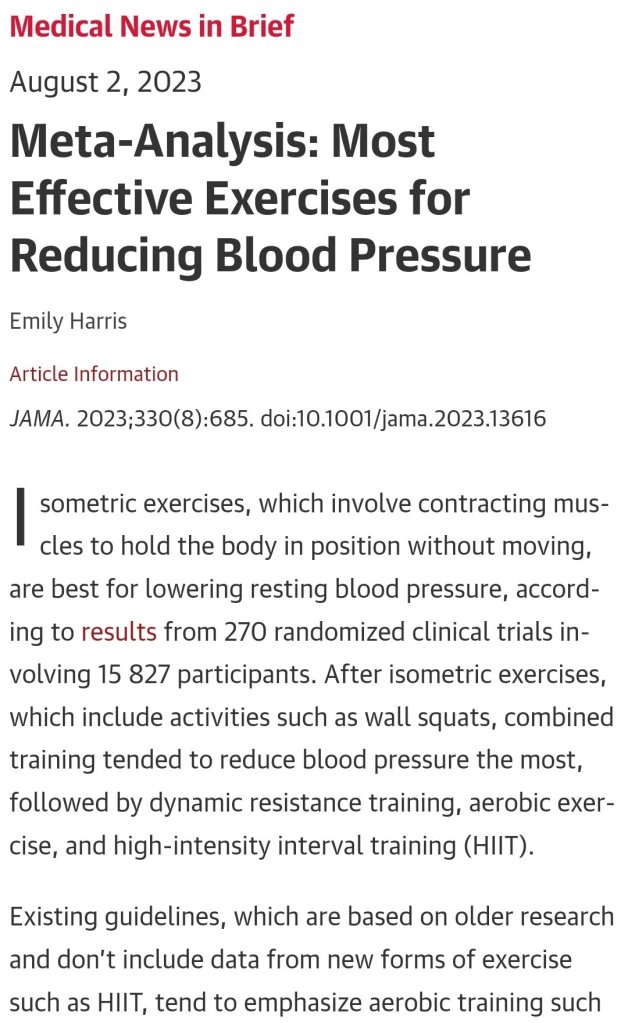
We (At least me!) have been taught, isometric exercise is not BP-friendly. In fact, it can cause intermittent spikes that may persist for a variable duration depending upon the basal as well as dynamic adrenergic vascular tone. This is what I had taught to my students. This presumption is nearly shattered by this meta-analysis. It concludes that among all, Isometric exercise reduced the BP more than others. (especially wall squats and planks). More surprising is, that the usefulness of aerobics is lesser than dynamic resistance training as well.
Final message
Contrary to popular belief, Isometric exercise is not really hard on blood vessels and is likely to have a more favorable effect on blood pressure than aerobics.
Still, hesitating to fully accept the conclusion of this study. Exercise prescription is highly individualized & includes multiple cross-over strategies and self-learning. Caution is required when doing strong isometric exercises, especially after a vascular event.
Reference