It is still a huge mystery, why the father of medicine stressed more about “not doing bad” than “doing good” .What made him to hold on to, such pessimistic thoughts , 2500 years ago . I am unable to think how he would react to this “tampered version” if he is alive ! My gut feeling is, he will find it hard to object .
Further reading (There is some debate , about the origin of this quote attributable to Hippocrates)
Diwali is celebrated today November 12 th, as “Festival of lights” an Important spiritual event in India, On this day, we pray God, knowledge, goodness, and peace replace Ignorance, evil and turbulence in this world.
Statins belong to a group of drugs, stolen and reengineered from the blueprint of natural Chinese red yeast rice (Monocoline K) in the late 1980s. The rest is the remarkable history in the pharma industry.
Statins directly interrupt the cholesterol synthesis by blocking HMG-CoA within the hepatocytes. It significantly lowers the LDL, fights human vascular atherosclerosis. It makes the plaque either regress, prevent progress, make it harder and in the process make them less vulnerable . There are innumerable studies that document the evidence. Statin has become a must-prescribe drug in any one with clinically established CAD or even in concealed CAD. Guidelines are available to prescribe statins various intensity, depending on the risk profile.
Which statin ?
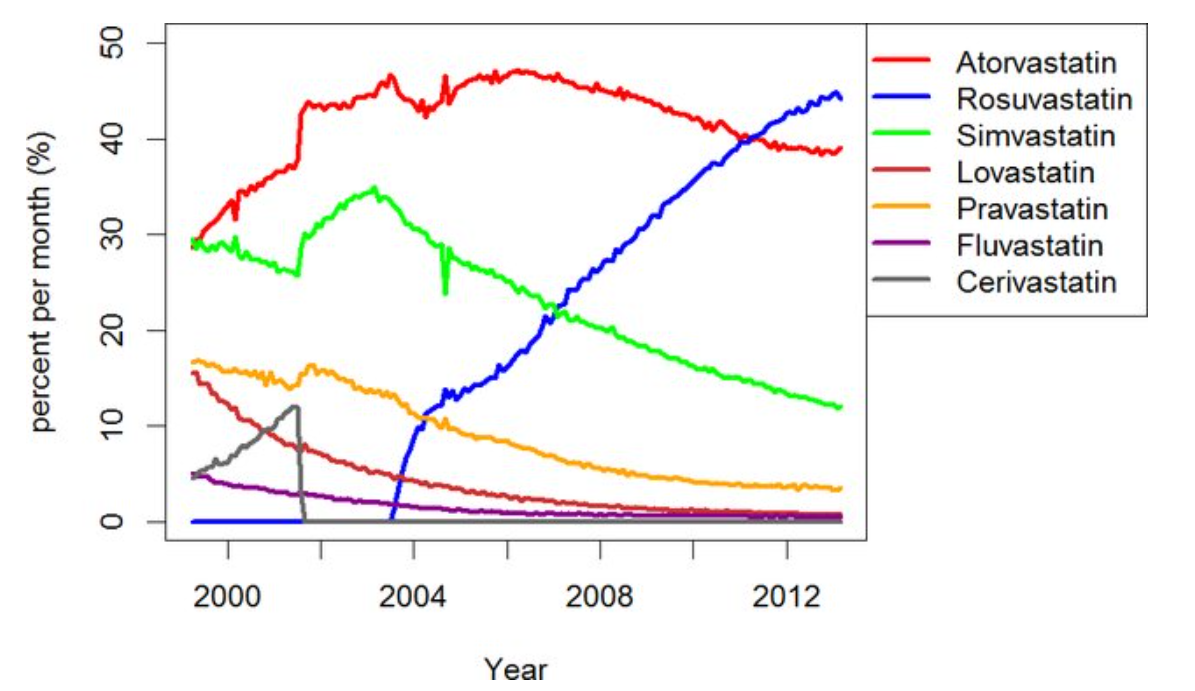
There has been a long list of statins. Many of them have retired from the ring .Currently, the fight is between Atorvastatin, a Rosuvastatin. Like Pepsi vs. Coke.
Note the graphic ,A meteoric rise of one drug since 2005 . (Can you guess the reason ?)
ATRORVA or ROSUVAWhich one should I choose ?
There is very little “one to one” comparison study between Rosuvastatin and Atorvastatin .The gap in the pros and cons are narrow. Following points are observed, without much dispute.
No one is dare enough to give strong verdict . Surprised to find one this month. BMJ has come out with a possible answer. It is called LODESTAR trial (Ref 1)
Mechanism of new onset diabetes with statins (REF 3)
It can be 7% with Rosuvastatin (less with Atorvastatin). We think, statins act primarily within the hepatocytes where cholesterol synthesis takes place, but they also have an eye on the pancreatic β-cells as well. It down-regulates GLUT-4 in adipocytes, and results in compromised insulin signalling. Furthermore, statins’ impact on epigenetics may also contribute to statin-induced T2DM via differential expression of microRNAs.
Mechanism of cataract with statins (Ref 2)
The cells lining that line the lens are dynamic and require cholesterol on a day-to-day basis. Statins inhibit proper epithelial cell development within the crystalline lens, where cholesterol biosynthesis is critical to maintain transparency and structure of the lens.
Final message
So, is it Atorvastatin or Rosuvastatin? It is left to you.
Mind you, “no statin at all” is the best option if circumstances and risk profile allows. Statins are never considered life-saving staple drugs in our fight with CAD and atherosclerosis. We, along with our scientists might may make you feel like that. Lipids can be controlled within desirable means exclusively with diet and exercise in most of the population* .
(*Forget about statins in the last 5000 years of known human existence, so many great people have lived a long and successful life in this world, without even knowing there is an organ called the heart that is responsible for the circulatory system)
This a story from a middle aged IT professional who had recently suffered from a cardiac event. His concern is, he has an ejection fraction (EF) of 45%, finds difficult to walk to the nearby mall ,while his neighbour, also a heart patient, has only 32% EF , but goes for cycling and hiking ! He finds this very odd and totally unacceptable. .He desperately needed an answer from his cardiologist.
How is this possible, doctor? I am sort of depressed for two reasons. You are saying, I had only a mild heart attack and recovered well with no significant blocks in the angiogram, but, I still find it difficult to do routine activities. The latest EF is recorded as 45%. I am taking all your medications sincerely.
“Doctor, I feel awkward, but I can’t stop asking this question to you. More than my heart condition,it is my neighbour’s one that is bothering me. He was critically ill sometime back. Has undergone a bypass, after two early stent failures, I am seeing him daily now. So active he is, able to hike even the hill in our county. He told me his EF is just 32%. It sounds atrocious. What is the use of having more EF than him, doctor ? Do you think I need to be referred to any specialized cardiac centre ?”
“My dear patient, relax. If you want a straight-forward answer, “you are suffering from EF neurosis” Exercise capacity and overall well-being of an individual have little to do with the Ejection Fraction (EF) of the heart. Forget that number”.
“Sorry doctor, I am not clear , do you mean to say I have a mental health issue? ”
Ok , let me go little more deeper for the sake of your understanding. Hope you don’t mind. EF% can be sort of the daily weather report. It can change even beat to beat depending upon the loading conditions of the heart. We, the cardiologists are partly responsible for creating this anxiety at your level with this number .The prevailing literature and the confused google , has misled you guys, to believe that EF% is akin to “bank balance” of available heart function. Let me apologize on behalf of all of us.
There are many cardiac and non-cardiac parameters that determine one’s exercise capacity. Lung function is vital. Systemic factors like quality of your Hb%, renal function, lastly, the most important factor, the status of your skeletal muscle structure and function. If I can go technical, the degree of LV size, associated MR, the stress of LV filling, pulmonary vein compliance, the way your lung vasculature reacts, RV function, degree of PH, all that matters.
In your case, each of these parameters is good. So, I can reiterate that your heart is in fairly good condition. It is most likely that your skeletal muscles are hibernating and taking too much rest, and their mitochondria are suffering from disuse. Further, your thinking pattern also makes you easily fatigued. You must also understand dyspnoea is a cortical sensory perception defect. It depends upon the behaviour of your cerebral centres that are localized in the amygdala nuclei.
“Please doctor, I expected a practical solution from you”
“Ok, let me tell you a positive proposal which will definitely help. Trust your heart and believe in my words and the drugs you take. Ignore this EF stuff. Send a friend’s request immediately to your neighbour and join him on his daily hiking. If he can do it, you can also do it. I expect ,both the issues that is causing you depression will vanish soon. One caution, don’t overexert. Stop 10 to 20% short of your maximum possible capacity.”
“Thank you doctor , I think you’re right I am not taking enough efforts and lack confidence .Will meet you again with good news “
Final message
Unless, it is extremely low contractile function, EF% has no linear correlation with functional capacity. This is the message to all those heart failure patients. Don’t feel bad if you are labelled as LV dysfunction or ‘Heart failure’. You can steal a success story from with the help of skeletal muscle training and dyspnea sensitization program (This is not a great new discovery, it’s all there in the ancient Indian medicine, it was called pranayama, a controlled regular breathing exercise)
Hypertension is a prevalent condition in the general population, as is mitral regurgitation (MR). For most of us, HT traditionally conveys a “singular meaning” that is, high pressure within blood vessels. We often forget that the origin of blood pressure begins right inside the heart, i.e, the left ventricle, which is guarded by two valves – the aortic and mitral. (Though we are aware, LVH is the classical response to HT),
Obviously, there will be signiifcant consequences to the structural integrity of these valves when LV pressure is raised beyond the tolerable limit of endocardial layers that line these valves. Mind you, the bottom of the mitral valve is whipped from beneath 100 tousand times times a day & 2.5 billion times in life time at an average pressure of 140 mmHg, and during exertion, it can reach up to 200 mmHg .Apart from hemodynamic damage, It should be noted MR in HT can be consequence of altered geometery duE to LVH, (Concentric Initially & eccentric in late stages)
The MR-HT link : Not to be missed
It is basic bed-side teaching that any isometric activity will push the blood from LVOT towards the Mitral valve, if it is leaking. Hence, it may not be a great discovery to show that HT will aggravate MR. Now, what is the new message you are trying to tell? There is big data (Really massive one, available from 5 million HT patients Rahimi K, et al 2017) that confirms with authority that HT patients are at risk of developing both primary degenerative and secondary MR at a later age.
If HT accentuates MR , why vasodilators didn’t show much beneift in MR ?
It is true routine vasodilators didn’t do much in regression of MR, but the subgroup analysis of those patients who have intrinsic HT or tendency of hypertensive response during exertion did benefit from vasodilator. So, it is mandatory that anti-HT drug titration is an essential strategy to arrest progression MR or prevent new onset MR.( Mojadidi M, JACC 2014)
Since we can’t selectively identify who will benefit from vasodilator therapy, it is always worth a trial of ACEI or even Amlodipine in patients with significant MR.(Note guidelines prohibit vasodilator therapy in MR unless it is Ischemic or non Ischemic DCM with functional or secondary) One clinical clue is, if a HT patient shows undue fatigue, one must suspect he or she is prone to develop MR on exertion as forward cardiac output is interfered with and fatigue results. (Special efforts must be taken to ensure a competent MV in HT patients) .
*Special effort means just a simple echocardiogram. In India, it can be taken for as little as $20 in any cardiac clinics or labs scattered across major cities. (Curiously, in Western countries, it costs $1000 and has a worrying waiting time as well, so it really becomes special effort!)
Assessing MR in echocardiogram: A well known tip
All of us know how tricky is, to assess and grade MR accurately. As discussed above it can as labile as systemic BP. Try to document the Heart rate and BP at the time of assesment.
Does Aoritc valve gets damaged with hypertension ?
Logically, high blood pressure is expected to damage the aortic valve more than the mitral valve. Does that happen? When the high-pressure ventricle contracts, the aortic valve is not resisting the flow like the mitral valve. It opens respectfully, so guess which valve is likely to get injured more. (However, it must be noted that the diastolic pressure exerts pressure on the far side of the aortic valve and can trigger aortic regurgitation and degeneration on the far side of the aortic valve. While high systolic jets can dilate or dissect the aorta. ) So, let me clarify this post doesn’t convey a meaning that Aortic valve is sort of protected against HT related Injury.
Final message
It is unacademic to delink mitral regurgitation (MR) from systemic hypertension, both in etiological and therapeutic aspects. Hence, it is wiser to include MR within the “Complication basket” of hypertensive heart disease. Recognising it and tackling in a timely manner will reap definite symptomatic benefit.This simple concept should be emphasized to our students.
A brief learning session with cardiology fellow about a possible new concept in Left heart failure.
What is the commmest cause for acute pulmonary edema?
“Left sided heart failure”
“Can you be more specific , Left sided means ?
“I meant LV failure , typically DCM of any cause or Severe un-controlled HT”
“Ok .good. Does Left Heart failure include mitral valve dysfunction also ?
“Yes sir, very much. Classical mitral stenosis and Isolated MR can cause pulmonary edema. In fact, acute AR Iis also part of left heart disease”
So far, so good, now coming to the complex part of left heart
Can LA fail in isolation independent of LV , ie I mean with normal Left ventricle ?
I am not sure. Can we call new onset atrial fibrillation as a primary atrial failure that can result in pulmonary edema?
Excellent. You are absolutely right. But I am talking about mechanical atrial failure, not electrical. Are you aware that most of the time AF is a well tolerated arrhythmia , it can even be silent in many cases. This is because the pumping function of the atria contributes only 20-25% to LV filling. This can easily be compensated by augmented LV suction force , provided the baseline LV function is normal.
Have you heard about ACM. Atial cardiomyopathy?
“No sir”,
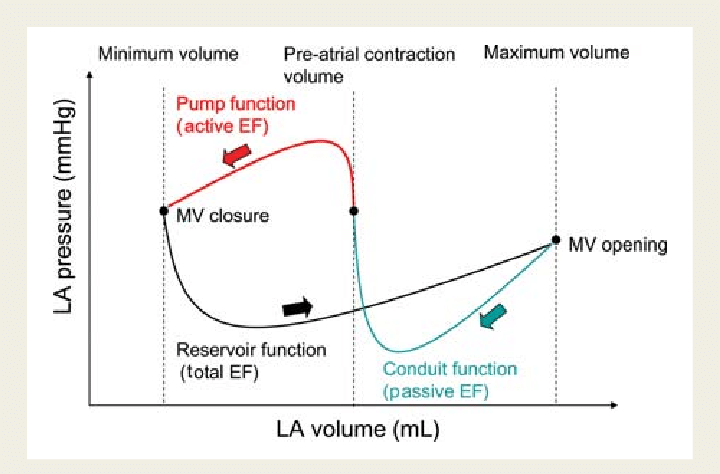
“You will hear more about it soon” (Ref 1) Scientists, especially Echo guys are closing in on this concept. We know, the atria has three functional components, namely conduit, reservoir, and pumping. Curiously, we have realized that the pumping function of LA may not be that critical from indirect observations from some land mark studies . (Rate control vs rhythm control studies in AF are a powerful proof on the atrial pumping function .(AFFIRM/RACE etc ) I don’t know, whether I am right in saying the above statement.
It is tempting to conclude , only if all the three functional components of atria gets affected , then only primary atrial dysfunction can be diagnosed. The concept is more complex than we realise. In diastole , pulmonary vein, LA , LV all work as single functional unit. Only in systole, we see them as different things.
Atrial DCM
Like LV systolic function, which is coupled with RV in parallel , LA function is closely knitted to LV in series during diastole. The key to suspect or diagnose this entity is to demonstrate dissociation of LVEDP with LA mean pressure & PCWP. This is not an easy job in bedside. Isolated Increase in LA volume without any reason , is one clue. LA ejection fraction is possible marker. (Kanagala P, . Int J Cardiovasc Imaging. 2020)
Final message
We are in the early days of understanding primary atrial mechanical failure, Atrial cardiomyopathy (ACM) or atrial DCM is being proposed as separate entity. It is very likely, some subsets of HFpEF might turn out to be primary atrial disease, depending on the level of investigation we do.
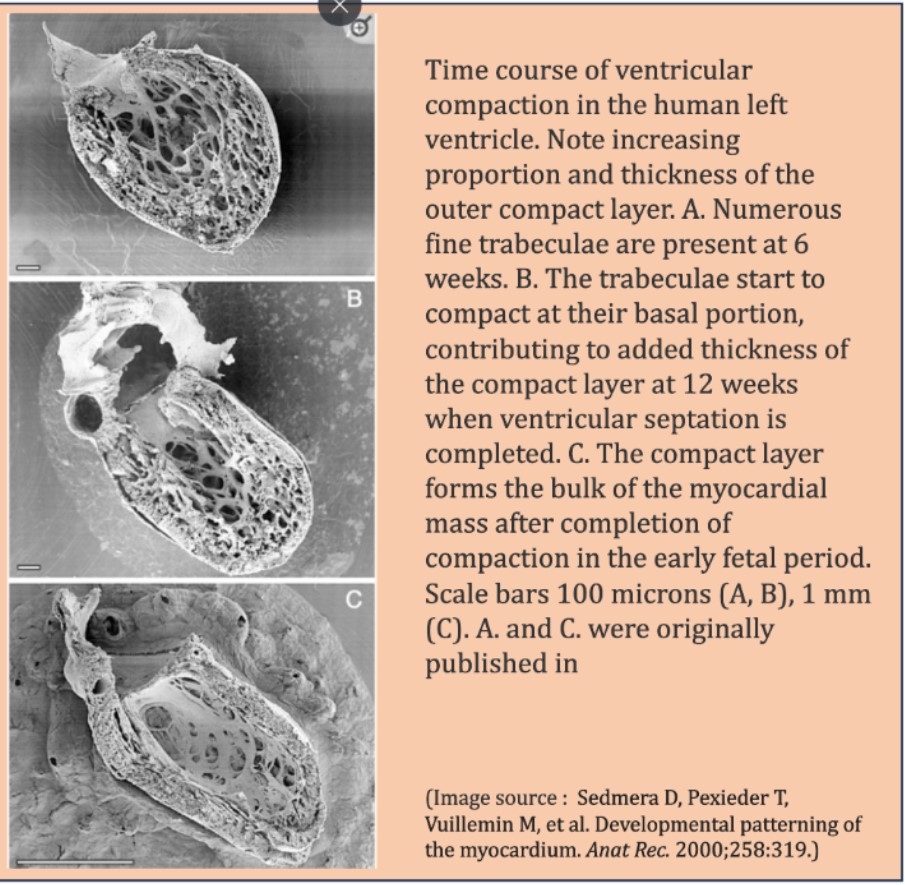
After formation of tubular heart , the initial increase in ventricular mass is achieved by development of trabeculations. Trabecular compaction coincides with genesis of coronary circulation, and results in formation of ventricular chambers.The hallmark of sponge-like myocardium is delayed and poor compactive forces.
Time line of ventricular compaction
A deranged compaction process need not be macroscopic. It can be very localized, regional, or global. The timing and the quantum of compaction is important , that injects the contractile power to the ventricle . It is increasingly observed in echocardiography that a small percentage of the population has more echo-free zones in LV myocardium than others. They could represent potential weak spots, at times of mechanical stress.
A curious case of normal Echo
Would like to share few images from a routine echocardiography in a healthy young female.
The apparent absence of mid myocardial shadow was not entirely a surprise though .At the same time, it raises some curious thoughts as to why certain myocardial areas are not well visualized by the ultrasound.
Look at the IVS, why should mid myocardium is echo free (measured 5mm) and appear de-laminated.
How echo is able to pick up only endocardium and epicardium , making entire myocardium look like an empty shell .
Still, LV is contracting vigorously, implying muscle mass is just not visible to ultrasound eye.
Clinical implication
These echo free dark zones in IVS or LV is so common, one can safely ignore, but its worth recalling few entities, that can be related to this. Intramyocardial hematoma, dissection and ultimately rupture (A case report) when they happen to develop an ACS -STEMI. We know , free wall and IVS rupture and mechanical complication occur signiifcant population of STEMI. Though, we can easily blame it on fate, may be these are the ones , who harbor such silent echo free slits due to defects in compacting genes making the myocardium soft , spongy that gives way wihtout a fight at times of tissue necrosis.
Can non-compaction occur without LV contractile dysfunction ?
Unlikely , is the likely answer from most of us. But , routine TTE might miss subsclinical LV dysfunction . We know , now degree of LV fucntion is directly related to the imaging modal;ity we depende to define it.
Can a consistency or sponginess of a myocardium be detected by echo?“`
As of now, it is not possible. This might become a reality when the science of tactile haptics enters the ultrasound domain.
Final message
“The act of observing changes the observed”
Non compacted LV is casually used term nowadays. The title of this post was made Intentionally provocative to stress a point, that what appears as non- compaction can be observed in normal persons.. However, request the fellows to look little deeper into the myocardial architecture, especially when you witness large echo-free zones.
Mind you, this is different from the well-defined condition of classical non-compaction with excessive deep trabeculations. Don’t know how to name this. This is different. Maybe “Isolated Intra-mural partial non-compaction” is an ideal term.
Counterpoint
When I discussed this with an expert colleague, he said, “No, you’re imagining a non-existing entity.” The ultrasonic interface with myocardium and the interstitial echoes that define the echo texture is so variable.Let us see.time will tell .(See this video and case report )
Postamble
This post is meant to be looked up purely from an academic perspective. Reporting such entities, unless you are absolutely sure, should be avoided, as it ends up increasing the anxiety of our beloved patients.
Cardiologists have always struggled to classify, assess, and grade one important valve disease, which is Mitral regurgitation. While valve replacement is the ultimate treatment, the timing of MVR is still a big debate. Apart from valve replacement, valve repair is a strong contender in selected patients. In recent times, cardiologists have made great strides to grab MR patients from cardaic surgeons. MitraClip, a percutaneous edge stitching , is possible with a varying degree of success.
Mitral valve edge-to-edge repair (MEER) is an interventional clone of Alfieri surgery that has shown conflicting results in the MITRA-FR and COAPT studies. The reason for this discrepancy in the MITRA-FR population is that they had larger-sized ventricles, which continued to pose challenges for the clip, which is focused only on the leaflets.
A new subdivision of secondary MR
Now, some of the cardiologists want to classify SMR/FMR into Proportionate vs Disproportionate MR. It may not be a great innovation, but it sub-divides secondary MR for optimal therapy. It simply says if LV dilation is significant, clipping the leaflet alone will not be sufficient; it would rather need an annular restriction either at the time of the index clip procedure or in due course. While Disproportionate MR implies, it is more of a leaflet coaptation defect, dominating over annular contribution.
Who proposed this ? What is the implication?
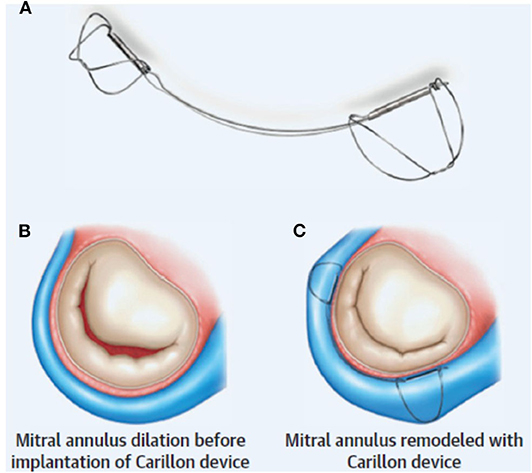
It is an afterthought, I think, from the makers of annular restriction device makers. MEER is found to be less effective in proportional MR.The Carillon device is a new arrival to tackle secondary MR .It is actually a wire that forcibly tightens the AV annulus inserted through coronary sinus . This modality takes advaantage of the aantomical proximity of coronary sinus to mitral annulus. Coronary sinus encircles and from a virtual wall along significant circumference of mitral annulus.
Unlike mitraclip, the Carillon device is claimed to tackle secondary MR irrespective of whether it is proportional or disproportional. It also has the potential to reduce LV dimensions in the long run. We have another device called IRIS-Millipede (to compete with Carillon).
We are free to have as many classifications in MR (Primary, Secondary, Functional, Atrial MR, & now Proportionate Disproportionate.) It is not the aim to bring up a rivalry between leaflet vs annular intervention. Ultimately, the most powerful component of the mitral valve apparatus, i.e., the LV muscle that matters.
I would request the esteemed researchers in MR ,not to keep EROs, regurgitation fractions, or chamber dimensions as primary markers of success of a device. Having strong clinical outcomes as the endpoint should be made mandatory, i.e., prolonging good quality of life and survival (But, the reality can bite hard. Someone told me, walking 20 meters extra in a 6-minute walk test is enough to get device approval from the authorizing entities.)
Recently, I visited a seven-star cardiology center. It had a fascinating lab with a near-360-degree roaming arm and floor (even the roof, I think!). The lab also had provision for optional thoracotomy support by surgeons and a CT scan. What’s more, I was told that an adorable robot will soon be added to the cath lab workforce to assist in delivering and maneuvering catheters. It’s truly amazing to see the advancements in science!
I asked the chief staff nurse how many procedures are being performed per day. She pulled out an Excel chart from a gesture-controlled touch panel. It was clocking about 20 to 25 cases per day. The lab performed the best of all procedures in our country. Great, well done, and congratulations, even as my lips uttered, my mind was thinking the opposite. Do we require such labs when the majority of the population struggle to get even basic medical care in emergencies?
Quantity vs quality of procedures
The said lab went on to achieve 2000 cases recently. It was crowned with glory in a stunning anniversary bash. We all take pride in numerical accomplishments. Quantity is easily measured. It’s simple mathematics. Assessing quality is a tricky one. Even professionally well-accomplished interventions may be of low quality.
Low quality and low impact may not be synonymous; still, it conveys the same meaning if we look at it from the patient’s perspective. The quality of the procedure shall be assessed with reference to the cost involved, clinical outcome, procedural as well as a perpetual chain of risk, finally, and most importantly the test of time.
Overall, the quality check of a cath lab is not only for the machines, it is also about the operators & what they do.
Postamble
Whover wants join this cath lab award session. Welcome .
* The winner was selected without any difficulty: No 3 : Its delayed PCI beyond 24 hours after STEMI (This accounted for 30 % of all procedures put together)
Meanwhile following competes for “high-quality” intervention
PTMC
Left the main/ proximal LAD stenting in UA/NSTEACS
Permanent pacemakers in CHB (Not all in SND)
ICD implantation for the truly deserving
RF ablation for AVNRT/ Some VT
Selected cases of Primary PCI
Some life-saving palliation in the newborn(Ductal stenting/IAS septostomy)
Diagnostic coronary angiogram in a strongly suspected ACS.
Choosing the winner was really tough, just leave it to the readers.
Final message
It’s worthwhile to go for such an analysis periodically to improve procedural quality & Impact. It’s wiser to allow our brains to prevail over hands. Global health is all about technology optimization, outcome analysis, comparative efficacy. The future sounds exciting though, with deep machine learning, data mining, skill transfer. However, there seems to be a definite risk. In the name of artificial intelligence, we might contaminate machines as well with humanness.
Let us restrict funding and stop Insurance coverage for low impact procedures. Instead, may use the resources for a truly life-sustaining & healing process.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.