
Archive for the ‘Uncategorized’ Category
Interventional closure of potholes outside cath lab with simple concrete device !
Posted in Uncategorized on October 29, 2017| Leave a Comment »
Ignorance based Primary PCI : A landmark article that couldn’t correct our coronary Intellect !
Posted in Uncategorized, tagged pPCI, primary pci stemi, st segment regression more important than ira patency, st segment regressionafter ppci, timi blush score, timi three flow on September 29, 2017| Leave a Comment »
How often you assess the success of Primary PCI with degree of ST segment regression or resolution ?
I posed this query to a freshly hatched , Intelligent and energetic cardiologist in an upscale dedicated heart care center.
He said, “No, we don’t .We always go with TIMI flow in IRA .TIMI 3 flow with less than 30% narrowing of IRA is success, that’s it ! He continued ,very often ,we don’t even Insist to take serial ECGs after the procedure . . . forget about analysing ST segment ! His body language seemed to suggest, he didn’t expect such a question (Silly !) from me , talking about ECG in this era of hyper Interventionism where we literally live within the coronary artery !
What a grave error in coronary cognition ? . . . thats commited day in day out of cath lab all over the globe !
TIMI flows across IRA lesion tell more about epicardial patency while the humble ECG reveals the true myocardial reperfusion.
So ,which will you use for assessment for successful reperfusion ? Ideally both , right !
But , as of 2017 ST segment regression is not considered worthy to define success of pPCI by the all powerful world scientific cardiology community .This is unfortunate (Or Intentional ?) we have ignored this Inspite periodic research papers showing the importance of the same. (Link to this land mark Brodie BR AJC 2005)
Do you know , none of the trials that celebrated the superiority of primary PCI in the last two decades used ST segment criteria. But then ,we realised much later even TIMI 3 flow can have near zero myocardial perfusion. So ,can we now say all these trials are invalid ?
We also never bothered to include no reflow as a liability during pPCI. We have enough data to say even restored No reflow during pPCI has worrying long-term outcome as reocclusion and tissue level perfusion is dismal .(Can we call it a pPCI failure equivalent ?) This is because the Cocktail of anti no-reflow drug we administer often give us a momentary satisfaction with transient myocardial blushes ! (Only to occlude minutes later as the patient is wheeled out of cath lab .We will never ever know how often this happens !) This is because , microvascular bed integrity is notoriously unpredictable and defies the conventional salvage time window . We have seen patients with ultrafast pPCI ending up with severe LV dysfunction.

Final message
If you apply the ST regression criteria by 90* minutes after pPCI (as we do for lysis ) the true success rate of pPCI will emerge .My prediction would be , if you do that routinely the hype of perceived superiority of pPCI might go down the drain (At Least in all low risk STEMI ! ) Let us do a large-scale trial comparing ST regression with TIMI flows, blushes ,frame counts etc and rediscover the true face of our beleaguered coronary microcirculatory sense !
*In fact ST regression should occur much early with pPCI than lysis (May be 10 minutes after restoring IRA patency ! )
Post-ample and a Quiz !
If coronary thrombus laden IRA is the chief culprit in STEMI battle field , Why is that Immediate , routine aspiration of thrombus in the ground zero is counter productive ?
That’s what the sophisticated mega trials of coronary thrombus TASTE, TOTAL revealed. I’m looking for an answer !
Reference
Counter point (and adding more confusion !)
Surprisingly , a Danish(DANAMI) study showed ST regression may not be Important in pPCI .This appears curious , especially when it suggests , ST segment regression didn’t occur because of more complete revascularisation by PCI !
Functional CT coronary Angiogram :Live coronary traffic Info on the go !
Posted in Uncategorized on May 28, 2017| Leave a Comment »
Technology is a great equalizer.Never in my dreams, I would have thought as I drive through the dense Nilgiris forest , a satellite located 36000 Km up in the sky would guide me through every turn and bend most accurately.

The curvy roads are coded with live traffic flow in Red ,orange & green . That’s “Google map” for you. (By the way, proud to note Google runs with an Indian CEO who hails from my city Chennai !)

Now , coming to academics , . .Some one thought, if the traffic in the entire globe can be monitored with few clicks, How about adding live traffic data to the otherwise dumb anatomical coronary angiogram images we get in a non Invasive CT scan ? We can even color code the different segments of coronary artery based on the velocity profile and pressure drop. That is CT- FFR . Now technology is available to get online live FFR as well. (Siemens )
Live coronary traffic blood flow
Heart flow the newest technology in coronary Imaging and non invasive Quantitative assessment is possible .It provides direct information about how to navigate the coronaries and intervene only the reddish areas leaving the greens untouched.
Principle
Its called computational fluid dynamics .A super computer calculates live FFR for the entire segment by measuring the drop in CT density data in Hounsfield units and translates into pressure equivalents and hence non invasive FFR.This modality has been approved by FDA.The heart -flow and Siemens has come out with onsite CT FFR.
Reality check :Have we conquered the coronary physiology ?
Trying to understand coronary flow with a engineering mind-set is Insulting the complexities of biology. Be reminded , Invasive FFR is assumed as a gold standard, Inspite of the fact that , its blessed with flaws in concept , techniques ,(Hyperemia vs no hyperimia) and lesional variation . Now ,what is the big deal , a non invasive CT -FFR is compared Impure gold standard and claiming a breakthrough ?
Of course,logic would suggest,if both FFRs are flawed why not use a less invasive one that is CT -FFR. It can atleast save time, cost, and potential procedure related issues.May be ideal in ACS situations were catheter FFR can destabilise the patient.Further, it can provide continuous live information in a hybrid lab , hence post procedure FFR is readily assessed . (Converting Red coronary into Green ones would become cardiologists new moto!)
Final message
The point of contention for the modern day cardiologist is ,they have realized (Not all ofcourse !) in a harsh way that , they must use a physiological confirmation of a lesion severity before indulging on fixing it with a metal. Whether CT-FFR will increase the number of angioplasties or reduce will remain a mystery . Whatever it does , it should do it for appropriate reasons . We know any technology has a shelf life and If MRI can provide the MRI-FFR (Journal of Cardiovascular Magnetic Resonance January 2014, 16:O55) , CT will be pushed back for obvious reasons (Prohibitive radiation hazard)
Reference
Good news for CT-FFR
NICE UK has approved the use of heart flow in its current guielines.
Status of MRI based FFR
Treat the Angiogram, not the patient for true benefits . . . oh, sorry do the opposite !
Posted in Uncategorized on April 11, 2017| Leave a Comment »
True patients* present with symptoms , please , don’t ever think all your patients bring their coronary artery for general servicing !
Ofcourse , we are the service provider to our patients . Though heart is a mechanical pump it can never be considered equivalent to automobile engine .
For a Heart service station equipped with 24/7 lab, the benefits may be more if you treat the angiogram rather than the patient.
Let us not misunderstand the word service , please show restraint, your patients will thank you forever.
* Silent significant CAD are indeed a problem in minority that requires selective wisdom.However, we can’t be aggressive hunters for CAD in population, as there is huge cost for human hunting !
Reference
Recent article which debates the issue of PCI in CTO
http://circ.ahajournals.org/content/135/15/1382?etoc=#sec-1
When do you use a tapering coronary stent ? Which company makes it ?
Posted in Cardiology -Technology, Cardiology Innovations, Cath lab Hardware, Uncategorized, tagged biomime morph long tapering coronary stent, lad coronary diameter tapers rca, long stent tapering meril morph, overlapping vs tapering stent, rate of tapering of coronary artery, Tapering coronary stent on April 2, 2017| Leave a Comment »
Coronary artery lumen has unique character . Its well-known LAD diameter is not constant , it tapers in its distal course.(Unlike RCA which is more tubular ) It is estimated LAD looses 15 % of its diameter for every 30mm length.Fortunately LCX has no such long course to make tapering a visible threat. (Though it may still be an Issue !)
Is there a hemodyanmic purpose for this tapering in LAD ?
Should be, God never designs anatomy without a physiological purpose.We have to find it out.(Can it be meant for flow acceleration as the flow is entriely diastolic in LAD while in RCA its both in systole and diastole ?_
What is the relationship between tapering angle and final distal diameter?
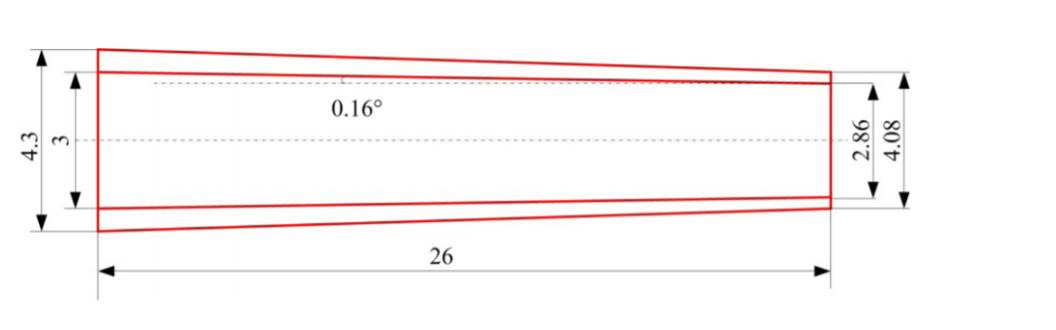
Schematic of an artery with a tapered angle of 0:16 .Ref XIANG SHEN Journal of Mechanics in Medicine and Biology Vol. 16, No. 8 (2016)
So, if you have a long lesion in proximal LAD and planning to stent with a 40 mm or long stent the distal end is hyperinflated by atleast 1.5mm, if we use a non tapered stent. Though , gain of extra diameter in distal segments might appear attractive, this may not work to our advantage , since it defies and distorts the natural hemodynamic flow pattern. Further , when you have tapering vessel, proximal optimisation becomes more important.
How about a tapering coronary stent ?
It should be a welcome addition to our already overflowing coronary hardware in fixing long lesions . Its still a surprise why only very few are making this type of stent.
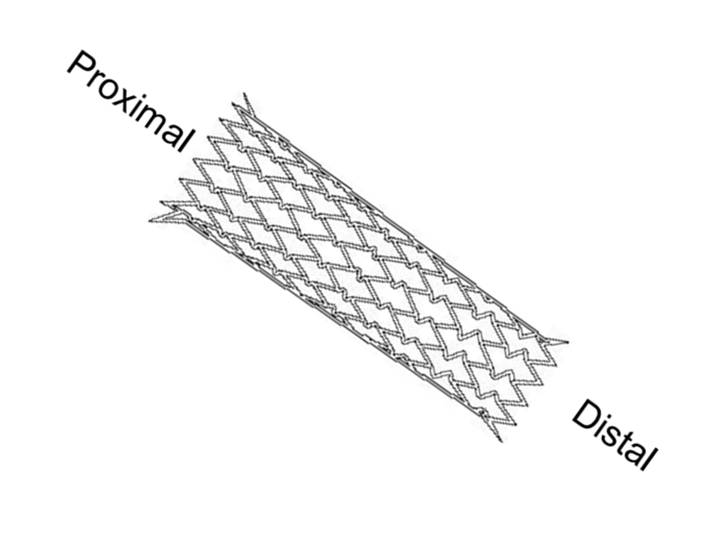
Meril has developed a tapered stent up to 60 mm long (Biomime morph).It should be useful in specific lesions sub types.Its worthwhile to note tapering stents are used more often in carotid artery .
Advantages of long tapering stent over two stents of different sizes.
- It avoid the vulnerable overlapping zone with double metallic load.
- Possibly cause less restenosis
- Low risk for stent fracture
- It reduces procedure time and of course the cost of stent by 50 %

Why the concept of Tapered stent is not that popular ?
I can only guess, probably lack of free availability and to a certian extent ignorance as well ! However ,current status about tapering stents is expected to evolve, though many cardiologist still feel it’s not clinicaly important issue to use a tubular stent in tapering vessel.
Alternative interventions in tapered vessel.
- Wall stent and other self expendable stents
- Tapered balloon Angioplasty (Laird Am Journal of card 1996)
Experts in this modality are welcome to share their experience.
Reference
When do you refer a patient from a “Higher” to “Lower” medical center ?
Posted in Uncategorized on February 3, 2017| Leave a Comment »
Medical practitioners often need to refer a patient from small clinics and hospital to a higher center for providing state of the art care provided by specialty hospitals armed with ultra modern Imaging , gadgets and devices.
Recently, I happened to see an elderly women with ca breast, radiculopathy, dilated cardiomyopathy, triple vessel disease , stented /by passed with 3 CABG grafts later, followed by an ICD and CRT, .Her CRT became non responsive after a failed attempted AF ablation.
.
After a prolonged stay in the posh AC suit of a renowned corporate hospital the patient was feeling exhausted and weak with multiple tests and procedure.The patient found things annoying as every consultant and support staff behaved like a programmed robots with artificial smiles and compassion.
She and her family was tolerating things, but desperately required a break from 24/7 attention (which was without much progress either ) . After a mini family confabulation, they decided to request the treating consultant to refer her to a lower center for a more humane care.
From here on its fiction . . .
The doctor agreed (after Initial amusement ) and asked his secretory to write a letter which sounded something like this,
Please get permission from the hospital desk for referring this 70 year old gentlewoman to a “lower health care center” as she feels exhausted with our treatment and decided to opt for a more simplistic, supportive , compassionate and humane care that’s is devoid of claustrophobic gadgets and machines .
We also acknowledge we are neither equipped , nor has personnel and expertise to provide that sort of human care, you demand ,! We have to respect science more than individual patient needs . We are taught, paid and live for science first ! so please forgive us.
But, we respect your concern and will transfer you to a primary health center.Thank you for being with us this long , and helping us the master some cutting edge skills and helped science to grow.

By and large, the concept of tertiary health care can very well be a myth.(With few exceptions) It means mechanised care that primarily involving aggressive organ specialists who want attack the disease without mercy for the patient.
The uttering here might sound provocative , especially for the families who have benefited from cutting edge medical technology , . . .
Still , the rate of growth of irrational organ or system based tertiary care is growing in dangerous proportions , and very soon we will realise the disastrous consequences of this pathological mindset of modern medical intellect.
What we need , ? Emergency bulk supply of “right and straight” thinking “whole body specialists‘ . Who are they ? they include the Internal medicine graduates ,humble general practitioners ,family physicians and geriatricians .These genre are currently in the sidelines suffering from artificial low self-esteem (atleast In India !) Soon I expect they should emerge stronger and take control of the sagging medical profession from the clutches of pseudo scientific specialty hospitals who keep the cost of medical care Insaningly high that drains the global GDP in a meaningless manner.
Will WHO act ? Should they be conferred the veto power and tightly control when to refer a patient from a lower to higher center and vice versa !
For those of you who don’t know who is who ?
WHO stands for World Health Organisation , a united Nation organisation which is the apex medical body & guardian of human health .One of their Job functions is ,they are expected to act when there is Inappropriate health delivery and expenditure .( Unfortunately even most of the medical professionals think WHO exists for only one reason to eradicate mosquitoes and vaccinate children ).
WHO need not think they exist only to guard health of poor under privileged , they have a critical responsibility to prevent wrong therapies committed to rich and affluent as well ! and more so these unnecessary modalities spill over from rich to poor in the name of equality !
Unexplained dyspnea post primary PCI : Never blame Ticagrelor !
Posted in Uncategorized, tagged drug Induced dyspnea, how does ticagrelor cause dyspnea, mechanism of dyspnea with ticagrelor, unusual causes of dyspnea on January 31, 2017| 1 Comment »
Knowledge can be a dangerous asset sometimes . A modern day cardiologist reassured a patient who had an unusual dyspnea after a muti-vessel stenting for a not so complex lesions following an anterior MI.The doctor was not mystified when the patient uttered this complaint. In fact he was so cool , reassured the patient since he was taking Ticagrelor ,and it’s well recognised to cause dyspnea in some patients.
Few days later patient called again and informed that the dyspnea is getting more intense and ultimately he was rushed to hospital only to diagnose subacute stent occlusion and a fresh ACS.
What do you learn from this story ?
Caution , extreme caution is required when dealing with symptoms following PCI and especially dyspnea.
A brief review about Ticagrelor dyspnea conundrum
- Ticagrelor ,a reversible P2Y12 blocker has a peculiar side effect of dyspnea (Which happens to be a cardinal symptom of heart disease as well )
- Its reported by up to 30 % of patients who receive it.
- It can be either exertional or even at rest.
- It seems to be dose dependent
- Onset within 24 hrs , upto 1 week.
- Pulmonary function not affected.
- Cardiac function thought to be unaffected.(No correlation with LVEDP though)
Mechanism of dyspnea with Ticagrelor (Presumed)
- Its direct cortical effect due sensory neurone P2Y12 blockadae.
- Due to Adenosine
Remedy
- Reassurance(Possible in few , but risky unless absolutely confident)
- Encourage Tea intake (Theophylline might nullify if its Adenoisine induced .
- Discontinuation is the specific option (up to 10%)
Final message.
Dyspnea is a unique side effect of Ticagrelor. Unexplained dyspnea is a delicately dangerous symptom in a post MI patient as it may directly imply a silent ischemia induced LV contractile dysfunction and acute raise in LVEDP.
Don’t ever take it easy and attribute all episodes of dyspnea to Tiacagrelor .If you are really not convinced consider switching the patient to a different anti-platelet drug. Its simply not worth for both patient and physician to spend anxious moments.
Reference
This simple question in Atrial Flutter ECG bothered me for long ! . . . Is the saw tooth upright or Inverted ?
Posted in Uncategorized, tagged cavo tricuspid isthumus atrial flutter, f waves in ecg, flutter circuit reverse typical, is it inverted or upright flutter waves, isthmus dependent atrial flutter, localisisng flutter circuit in ecg, mechanism of atrial flutter on December 1, 2016| Leave a Comment »
We know, classical Atrial flutter (Also referred to as typical /Common AF) records saw toothed F waves due to continuous atrial electrical activity across a macro- reentrant circuit within right atrium.
Though this saw tooth pattern is easily recognised , it’s often difficult to say whether the saw is facing upwards or downwards ?
ie Is the flutter waves are inverted or upright ?
The general rule is the shallow stroke (one with a lesser slope) is to be termed as antegrade / initial deflection that will determine the direction of flutter waves.

This is because , the forward limb traverses the slow path of the circuit namely the cavo-tricuspid Isthmus, it then ascends up in the inter atrial septum (There by inscribing inverted F waves in leads 2,3,aVF .The return circuit is relatively fast, crossing the antero -lateral free wall right atrium and hence the later half saw tooth has a sharp deflection )
In Reverse typical flutter the flutter waves are upright (with a shallow slope ) in inferior leads but still uses the cavo- tricuspid Isthmus
* Note: In lead the polarity of F waves in V1 it will be opposite of that of inferior leads.

Why should we bother about direction of flutter waves ?
It may not be important for those hifi EP guys who can ablate complex arrhythmia with intra cardiac GPS catheters and accurate electro anatomic mapping system. Still , the surface ECG always help us understand the basic circuits of flutter.
Reference

Reverse typical flutter should not be confused with atypical flutter where typical saw tooth waves are uncommon.The later group is termed as atypical atrial flutter that arises from various other focus including left atrium.
What ails cardiology literature ? Watch out . . . Guidelines may easily misguide you !
Posted in Uncategorized on November 21, 2016| Leave a Comment »
If you think , the various appropriate use guidelines for cardiology practice are collection of great scientiifc truths , beware . . .many of them hide behind semantics. (After all , English is an unique language one can play with it !)
Is it not funny , to note a recommendation that goes with a caption “may be appropriate” conveys exactly the same meaning as “may not be appropriate” as well .
Here is a rare article which tries to expose the importance of linguistic Interventions in cath lab that can Impact the patient outcome for good or bad.
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- March 2026 (6)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,637,299 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note


ORBITA trial : First let us do some harm . . . second , we shall . . !?
Posted in Cardiology -Interventional -PCI, Cardiology -Technology, Cardiology -Therapeutic dilemma, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology journal club, cardiology wisdom, Medical education, Medical ethics, Uncategorized, tagged ABUSE OF STENTS, ACC AHA ESC ORBITA GUIDELIES, CHRONIC STABLE ANGINA GUIDELINES, drsvenkatesan, HOW ORBITA TRIAL WILL CHANGE MY PRACTICE, INAPPROPRIATE USE CRITERIA AUC STENTS, LANCET ORBITA STUDY, ORBITA COURAGE BARI2D FAME 2, ORBITA IMPERIAL COLLEGE, ORBITA study, ORBITA TRIAL LANCET, ORBITA trial review and comments, ORBITA VS COURAGE, reviewing ORBITA trial study critically, TCTMD 2017 ORBITA, WAHT WE LEARN FROM ORBITA STUDY on November 6, 2017| 2 Comments »
Cardiologists at confused cross roads !
Perils of limited Intellect & Infinite greed
When not so appropriately trained cardiologists do Inappropriate things “use becomes misuse” . . . then, it won’t take much time for science to become total abuse. That’s what happened with the murky world of coronary stents .No surprise, it’s time to firefight the healers instead of the disease !
Now ,Comes the ORBITA study . Yes , it looks like a God sent path breaking trial that spits some harsh truths not only in cardiology, but also in behavioral ethics .Let us not work over time and hunt for any non-existing loop holes in ORBITA. Even if it has few, it can be condoned for sure as we have essentially lived out of flawed science for too long Injuring many Innocent hearts !
Yes , its enforced premature funeral times for a wonderful technology !
GIF Image courtesy http://www.tenor.com
Meanwhile, let us pray for a selective resurrection of stenting in chronic coronary syndromes and stop behaving like lesser professionals !
Postamble
Extremely sorry . . . to all those discerning academic folks , who are looking for a true scientific review of ORBITA , please look elsewhere !
Rate this:
Read Full Post »