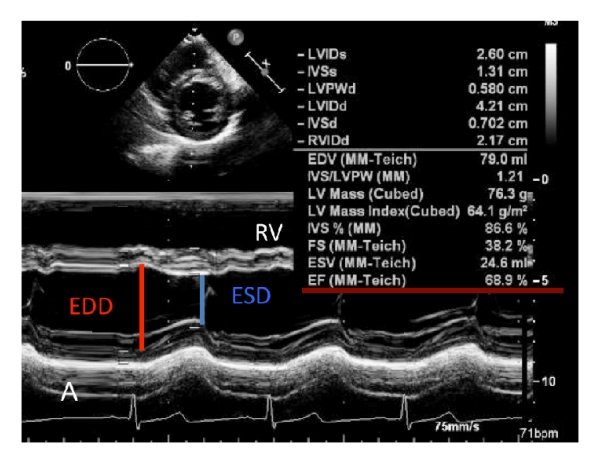
Which point in ECG is taken as reference for End systolic dimension for LV function assessment?
Marking the end diastolic point in ECG is quiet straight forward. Peak of R wave.(or Q)*
But, what about the reference point for end systole.
Descending slope of T wave
Peak of T wave
End of T wave
If T is absent or not clear , I will be confused
To be realistic, ECG has no reliable reference point for end systole.
Answer: If I say the answer is 5, no one is going to agree. Please note, the relationship between the T wave and the peak systolic phase in echocardiography is weak. Is there any relation at all ? Then, how to measure LV function in echocardiography? There is a electro-mechanical delay in every segment and sequence of cardiac contraction and relaxation, with former piping the later (electricity beats).
Surprisingly (illogically as well), we take the point of maximum thickness in M-mode as end-systolic, which, in fact, corresponds to peak mechanical systole. This point has no consistent relationship with any part of the T wave. We must realize, the clinical cardiac cycle is defined based on sounds, i.e. S1 and S2, while the biomechanical cardiac cycle is different. Similarly, echocardiographic systole is not the same as clinical systole. 2D echo eliminates this uncertainty to a large extent. This is one of the reasons , we are advised and encouraged, not to measure LV dimensions in M mode.(A very tough advice to follow though)
Final message
We are not completely clear yet, in the “ECG vs Echo” time correlation of hemodynamic events. The errors may be in only milli-seconds, still, when planning for Interventions like re-synchronisations, and in the follow up of DCM patients this could matter much.
Learning resources in the web, has made the traditional methods of learning & teaching almost redundant.
American society of Echocardiography (ASE) has produced this 20 page PDF document, which covers the entire field of echocardiography , in an Illustrative format.
Take a print out, of this and stick in your lab (If you have space) for an Immersive experience. Hope, sharing this document here doesn’t violate any copyright issues.
Answer : Is the coronary dissection really painful ? As in most situations of scientific medicine, the answer to the question is, It “may or may not”. But, for some strange reason, it is more often painless . Mind you, even if it occurs, it is atypical, continuous, non-anginal if flow is unaffected, and not relieved by nitro-glycerine. This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , may be misdiagnosed as post infarct angina.
Spontaneous coronary dissection vs Iatrogenic dissection
SCAD is a rare , different entity , enjoys a popular space in the patho-physiology of CAD. it is a disorder more common in women, especially in pregnancy where hormones tend to soften the connective tissue in vascular EC matrix. An important therapeutic caution is PCI is contraindicated in SCAD except in critical locations such as left main.
Answer : Q 1: A / Q 2: C. It is indeed a physiological molecule in small amounts that help carry hormones across the blood. In pathology, it accumulates in huge amounts. It is a disorder of protein folding, making them thick, stiff , sheets of peptide, hence mis-behaving with adjacent cells, injuring them in the process. This is responsible for the systemic nature of disorder right from the brain to peripheral nerves, Heart, kidneys, liver, spleen, etc. (Ref 1)
(*It should be stressed , majority of deposition occurs in extracellular space.They clog the interstitial space, also can invade the cell, especially in neurons in Alzheimer’s disease . Now we have evidence that Aβ (A beta) get into the myocytes as well. (Troncone L, J Am Coll Cardiol. 2016) Fellows, better say amyloid is primarily extracellular, but, by pressure effect and injury of cell membrane it results in cell death.)
Till now, these disorders has been termed as a degenerative disease with no viable options. Now, we have made a breakthrough. A group of drugs genetically created work by unfolding the proteins by interfering with RNA (SiRNA) that home in on the host liver and help clear these systemic proteostasis, the key pathology in Amyloidosis (TTR).
Patisiran is approved by FDA for peripheral neuropathy and used in cardiac amyloidosis. Patisiran is a siRNA encapsulated within a lipid nanoparticle delivery system for targeted delivery to the liver, the primary source of serum TTR . Once in the liver, siRNA binds to the untranslated region of TTR mRNA and degrades it, inhibiting TTR synthesis. ( Adams D et al NEJM 2018)
Many times , an Innocuous question poses a real challenge, to our life time understanding of circulatory physiology.
This question is very important , if we want to understand the true mechanism of postural hypotension, a commonest autonomic disorder in elderly (& also the newly recognised entity orthostatic hypertension)
Mechanism
Orthostatic hypotension is defined as a sustained drop of at least 20 mm Hg in systolic blood pressure (SBP) or 10 mm Hg in diastolic blood pressure (DBP) within 3-5 minutes of going from a supine to a standing position. In patients with associated supine hypertension, the criteria for orthostatic hypotension allows for a drop of at least 30 mm Hg in SBP or 15 mm Hg in DBP.
Can you discuss the answer to the question please ?
The correct answer is likely to be this. In normal adult, the systolic BP falls and diastolic BP is either static or raises by few mm . DBP is never expected to fall on standing, as the fall in systolic BP is invariable, that trigger a vasoconstriction which will increase the PVR and make sure the DBP doesn’t fall. In the process mean BP is kept near normal and regulated.
However, hemodynamic response to standing has no fixed rules. That’s why we keep definitions, like acceptable fall in systolic and diastolic BP . It depends on , age , central and peripheral neurological nervous system, preconditioning of vascular tone.(Not only arteriolar, even the much neglected venous tone).
For the seekers of evidence, there is one study which was specifically done to find orthostatic BP response .(Smith et al Ref 3) .It highlights the point, the immediate vascular response ie (<30sec) is totally different from prolonged standing, Implying, the response time of even an intact autonomic nervous system can be quiet variable.
Obviously it will add on to the complexity, if we say there are common roots in pathogenesis between the two entities. It is indeed true. Both comes under the basket of dysregulated autonomic nervous system. Please recall , we have a condition called supine hypertension and standing hypotension , POTS syndrome etc that should stimulate us to search for those hidden secrets.
As the name itself suggest, autonomic nervous system has its own control(or no control ) with a complex and poorly understood brainstem and cortical network. This operates through physical wiring directly as cranial nerves or piggy packing along the spinal cord tracts , vascular tree, and somatic nerves. The biochemical orchestra of this system is played by a delicate balance of adrenergic vs cholinergic forces.
Next question
What happens to BP during exercise ?
This again has more dynamic and interesting changes especially in the diastolic BP .Read Guyton’s physiology or the good old Rushmer’s hemodynamics monograph, linked in this site elsewhere.
“Yes, it is true. It is tough to consider oxygen as a “powerful and magical drug”, because it is freely available everywhere.”
Routine nasal Oxygen has little use in the management of STEMI. In fact, it can be harmful as it causes vasoconstriction. Hence current guidelines, has very strict advice about not giving oxygen unless systemic tissue hypoxia is documented.
Now, how about infusing Liquid oxygen right inside the LAD , the target zone , that is hit by hypoxia.?
This is not a new concept. G.W. Stone et al. tried this in 2009 itself.(Ref 1) For some reason, this was not followed up. How did we ignore basic fact myocyte hypoxia require Oxygen at that level. We were concentrating to reperfusing with blood, but what the cell need is not blood b but oxygen. Now,14 years later, some young researchers reaching out to this concept ,via liquid myocardial oxygen . Hope to be a possible breakthrough success .it was presented at the 2023 SCAI meeting in Phoenix. In this study, a 60-minute intracoronary infusion of liquid oxygen after pPCI reduced the infarct size and arrhymic risk .This study was sponsored by ZOLL® TherOx® .
A possible deterrent is the problematic and complex concept of reperfusion Injury. The term Oxygen radicals always sounds sinister .Really I can’t understand how a cell which get injured by the lack of a a particuar gas, get damaged by the same gas .(Oxygen in liquid from might behave differently as in this study ?) I think,its all in timing of delivery of oxygen, and if we start thinking like Einstein, then ,there is nothing called time.
Innovation and experimentation is must be allowed as liberally as possible. Breakthroughs happen accidentally at any time. Systemic oxygen may be harmful, but localised delivery of O2, might exactly be the thing, the dying tissues are waiting for. Sometimes we Ignore a good concept for no reason. Bias against drug companies also can be counterproductive.
Now, you can view who all are reading this site live on a revolving globe. It makes all the more happier to note that all these grateful and honourable dots (i.e., you) are literally drawing the world map . Six million reads from 190 countries, right from the Solomon Islands in Micronesian Pacific, abutting the International date line, to the extreme west, reaching Chile and Hawaii has happened so far.
A casual read of the original paper threw up some thoughts.
India’s apex medical body, ICMR, initiated a study primarily on sudden deaths among young people in covid times . The primary intention of this study was to find what causes sudden unexplained deaths . and also test the hypothesis that the deaths were not probably related to covid vaccination. The study did prove that. (I am not an expert to assess the statistical validity and scrutiny of the study. It is too complex a model. Still, I do have a primitive query as shown in the title )
But, we expected a minimum revelation. What caused these 729 deaths (filtered out of 29000 deaths) I understand physical autopsy could not be done in majority of deaths (Even in witnessed , in hospital deaths). So, the question remains . Is it sudden cardiac death ? Is it sudden “non cardiac ” death ? or can it be a “non sudden” masquerading as sudden in any way.
Though this is not a hypothesis-proving study, it is apparent that the intention of the study primarily revolves around removing the stigma and fear associated with vaccination. (The fact that only a fraction of patients, (less than 2%,) were hospitalized for COVID indicates that this study primarily intended to test the risk of COVID vaccination, which was around 85% in both groups.) It makes sense, for the study group , they created a good methodology accordingly and indirectly proved the hypothesis right. As physicians and cardiologists, we wished also look into the data of what caused these deaths by performing autopsies in all possible cases. The results of these autopsies need to be known.
Conclusion is fair
It is traditional (and acceptable ) to blame the heart for all unexplained sudden deaths. The study suggests that heavy drinking, along with with intense physical activity in the background of positive family history, is behind many of the deaths. It is a fair assumption that they are all cardiac. Sudden neurological and pulmonary deaths are under reported. In fact many of the SCD is an arrhythmic event originating from CNS or electro-ionic triggers in blood with the healthy heart
Is this not a major limitation*
When you want to know whether COVID vaccination is related to sudden death in any way ,is not ideal, weneed to have a control /cohort arm who have had no vaccination? In this study, both groups had nearly 82-88 % vaccination. In fact, the control group had few percent extra vaccination, and this helped the study, to claim that vaccination prevented some of the sudden deaths. This seems far-fetched with any statistical methodology. This, I feel is a serious limitation. It can even nullify the study conclusion to a large extent. (Experts please clarify , It may be an entirely wrong perception and lack basic knowledge in statistics.)
One more possiblity , can we combine a case-control study with add on accessory cohort and follow up as a dual mode study ?
Final message
It is a landmark attempt to study the mysterious deaths among young Indians in covid & post covid times. Two things .This study can talk about only vaccinated population. Does this study prove, people who have not vaccinated had more or less sudden deaths ? No. this study has no scientific grounds to talk about either positive or negative status of unvaccinated population , because there is no, unvaccinated cohort and follow-up.
At the end of the day, an unexplained death remains unexplained because we couldn’t do autopsy (Of course we have found the same known risk factors responsible , except probably new one vigorous physical activity , )
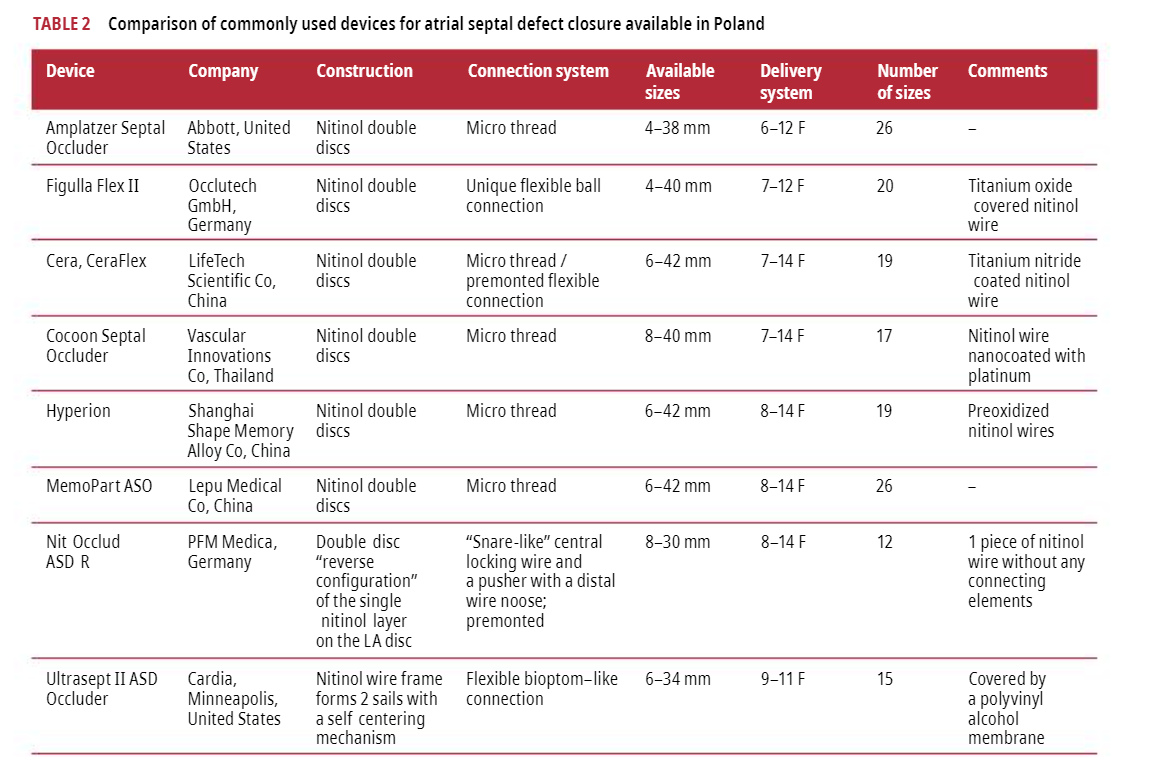
ASDs are classically oval, but devices are typically circular.(Exact Incidence of ovoid ASD is not known. but it easily exceed 50 % .(Recall, the embryologically ill-fated hole expands around the fossa ovalisnot circularis )
Do we have Oval devices ?
I think, we don’t have one . Please check from this list , a good document on ASD device implantation from Poland
Why do we accept this shape mismatch ? What are the potential issues because of that ?
When closing non-circular ASD, the size of device should be considered according to the multiple diameters of the defect. One diameter of the circular device could be too large for the shortest diameter causing a deformity in residual rims. The cardiac erosion after successful implantation as one of the most important complications due to a larger device in the oval defect compared to the circular defect (This text was taken from (Ref 1)
Why the idea ovoid device was never popular ?
Technical issues in sizing the exact oval defects ,device company’s lack of interest. However, designer devices with perfect fit with the help of 3D printing is very much possible.
Is it true ,an Oval device might hold good even in the setting of deficient IVC or posterior rim ?
May be. Some truth in it. I am not an expert to comment.
Do we really require a perfect fit devices ?
When I discussed with an expert , he said there is no need for oval device . A large circular device 2mm larger than the long axis diameter of the oval orifice is not an issue at all . Some how, find it difficult to accept that. What about you readers ? Please respond if you have any comments.
Any study on this issue ?
Yes. one study specifically looked into this. It compared the effect of circular device on oval defects. It concluded there no difference in any adverse outcome , but oversizing is unavoidable with oval defect.. This study , though addressed a vital query ,is never meant to find the truth we want, as it has no oval vs circular device to compare the outcome.
Final message
It is strange ,cardiologists look for perfection and precision in every cardiac intervention, … while in case of ASD device closure, size is sacrosanct,but shapes, we are allowed to shrug off. May be things will change.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.