
Subscribe to continue reading
Subscribe to get access to the rest of this post and other subscriber-only content.
Subscribe to get access to the rest of this post and other subscriber-only content.
Posted in Uncategorized |
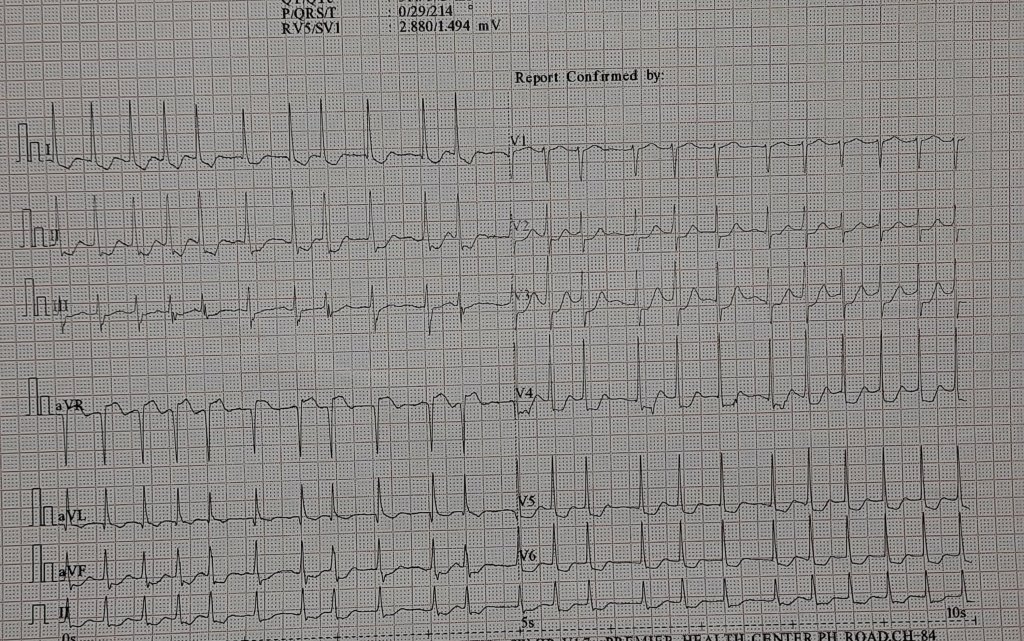
ECG diagnosis any one can make. The second part of the question needs some thoughts.
Dissecting the ECG* diagnosis
1.It is Atrial fibrillation with fast ventricular rate, with signifcant ST depression in V 4, V5, V6 .This could Indicate few things.
2.Preexisting LVH with AF
3.AF with new onset ST depression. This would mean an emergency (or may not) if it is an thromotic ACS high risk UA with posssible left main. But, one should bear in mind AF is an Natural atrial stress test , and ST depression could simply be a marker of tight fixed, stable lesion, (without a thrombus) that would require an elective Intervention.
4.Coming to the The ST elevation in AVR, many strongly believe it is a marker of left main disease. (Still, we can’t call it as AVR- STEMI, because it may just represent reciprocal ST elevation to any sort of ST depression in lead V5/V6 that includes benign LVH )
5.Look for ST elevation in lead V1 whenever you have ST lifts up in AVR. If V1 is isolectric , left main is very unlikely
The second part of the question.
I am sure, ruling out CAD without angiogram will be labeled as outright crazy. No cardiologist in their right sense will do that, I guess. Still, we could do it in this case. What did we forget in this discussion so far? We got lost in the electrical debate and failed to address the fundamentals. Why did this patient come to the hospital, requiring an ECG?
What did the clinical examination reveal?
While the cardiologist could not rule out CAD, the calm patient, complaining only of palpitations, ruled out a potential emergency chain reaction. Furthermore, a crescendo murmur in the aortic area sealed the issue. Yes, it is moderate aortic stenosis confirmed by an old GP’s prescription slip. She is being evaluated again for the severity of AS, treated with rate-controlling drugs for AF, since there was no acute heart failure or angina.
One more question
Why AF is not precipitating left heart failure even in patients with aortic stenosis ?
The concept of Left atrial functional reserve is a seperate topic, that will answer this query.
Final message
You don’t require an urgent cath lab mobilization to rule out CAD, even in a patient with a frightening ST segment, stuttering amongst irregular tachycardia. Always listen to the patient and have enough patience to look into the old records.. For that, we need to realize, we have to allow the patient to talk.
Postamble.
Presence of AS in no way rules out a CAD.Both can co exist. But if severe AS occurs with significant CAD, absence of angina is exceptional.
Posted in Uncategorized |
World heart day is being celebrated every year on September 29th ,Initiated by the World heart federation with a genuine purpose, vision & goal. It has become big hit in recent times. In India, the theme has captured the imagination of the main stream media . Every one wants to propogate a message. I am not an exception. Please bear with this skewed message “One for the patients and the other for the self” !
Posted in Uncategorized | Tagged acc aha esc, ethics in cardiology, lancet, medcial education, nejm, right treatment movement, world heart day, world heart federation |
Interventional cardiologists generally do not believe (rather relish) in simple balloon dilatations to remove any vascular blocks. It is a mundane job for their talent-rich hands. After conquering the coronaries, we made exclusive valvular stents. No surprise, TAVR has taken over the aortic interventions with all its glamour and vigor, though it is definitely not an ideal choice in all.
SCAI, the prestigious journal in Interventional cardiology has a recent article , that has a not-so pleasant message for TAVR lovers.

Very soon, BAV could pose a direct challenge to cardiologists’ heart throb TAVI. Though, it suggests BAV as an adjunct or bridge , there is every reason to belive the bridge can outlive the lives of many co-morbid subsets in TAVR eligible cohorts. (ACC 2014 guidelines already has a grossly under-rated 2B/ Evidence C Indication for BAV)
It seems reasonable to believe BAV, with considerable improvement in hardware, technology, and expertise can be an alternative to TAVR in high-risk aortic stenosis in a substantial number of patients.
It is also worth pondering over a less discussed aspect of BAV. The apparent high adverse events with BAV in calcific AS reported in the past-PARTNER days are now proven to be either exaggerated, outdated, or outright false. (For the evidence seekers, there was never a control BAV arm in none of those big studies on TAVR. It was purely a Surgery vs TAVR study. (A flaw in the aim of the study?) They may call it unethical to have a BAV limb, my understanding is, the absence of which is more unethical, as we claim superiority of TAVR without a less invasive option of BAV as control )
The fact of the matter is, in many centers, the risk of sudden death or acute aortic regurgitation is either comparable to or acceptable when compared to transcatheter aortic valve replacement (TAVR). It is worth emphasizing that BAV can be performed regardless of the load and location of calcium, while TAVR requires minimum elastic calcific load assistance to hold the valve in place. Further, BAV-related issues can now be effectively managed with efficient hemodynamic management.
Final message
If not scientiifally discriminated*, new age BAV can upgrade itself from the “self imposed contraindication” to, a sustainable alternative to TAVR ,atleast in selected sub-group of patients with isolated AS. This reality sould be perceived not only in the cost perspective, but also in the overall superiority in avoiding all those menacing complications with TAVR.
Postamble
*Very difficult task for the humble balloon to prevail over glamarous TAVR. Still,there is some hope(.We can get it from the emerging DEB story, where balloons are able to get rid of stents from the coronaries).
Reference
This is an interesting and important paper in the BAV vs TAVR debate. The funny thing is, even after reading it twice, I am unable to clarify which procedure this paper really favors!
Posted in bav vs tavr, TAVR, TAVR /TAVI, tavr tavi, TAVR VS SAVR, Uncategorized |

Postamble
This quote is being sent for the annual meet of “Right care movement” I know ,this can sound outrageous, permissble limits of abuse ? Up to 2% or 5% ? Let it be anything . Meanwhile try to enlighten yourself , the key differences between misuse & abuse.
Posted in bio ethics, Medical education, Medical ethics, medical satistics | Tagged best medical quotes, bmj, dr venkatesan sangareddi, first do no harm primum nocere, hippocrates, Hippocratic oath, inappropriate medcial care, jamanetwrok, lancet, madras medical college, medcial ethics, medical science future, nejm, nobel prize in medicine, over treatment, principles of practice of medicine, william osler |
Discussing lifestyle modification is an essential cliché in every preventive cardiology consult, For most, it still means good nutrition exercise, and stress relief. It is true, that the average human longevity has increased considerably in the last century. However, this apparent gain in life expectancy by the stunning discoveries in science ( 10 years ?) has already been eaten up, by the self-inflicted, poor styles in life. The new kid on the block, i.e. social media is playing a powerful amplifying effect.
Spot a new entry in lifestyle interventions.
Here is a fresh list of lifestyle modifications from the latest edition textbook of heart disease by Dr.Braunwald, considered the bible of Cardiology. Not at all surprised, to note the new entrant at the bottom of the list.
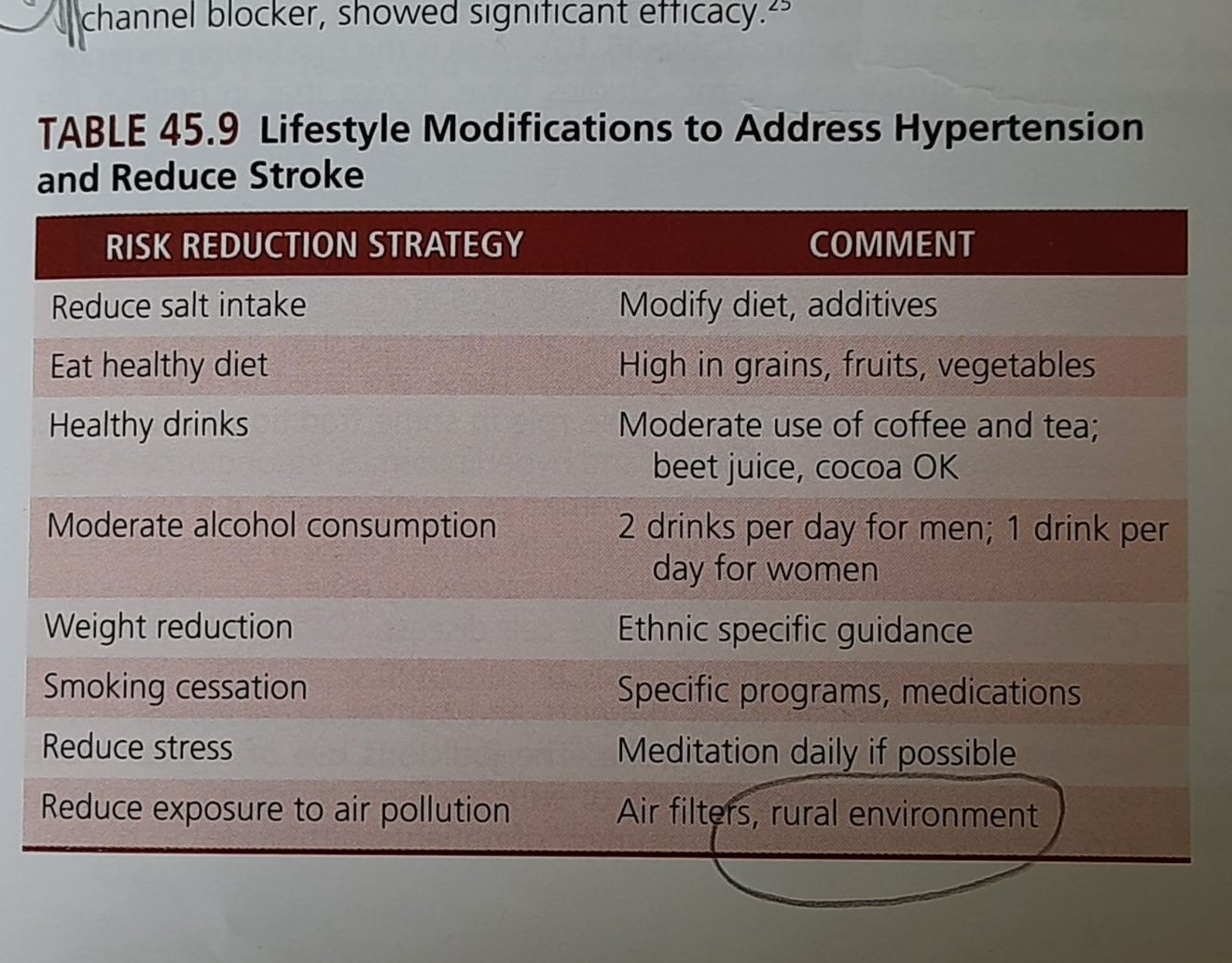
Yes, It is asking us to consider moving out, from the lovely city life to the countryside, and gift a pure and peaceful life to our vascular endothelium, which is devoid of PM2.5, NO2, Carbon monoxide (CO) Sulphur dioxide (SO2), etc.
Final message

I would expect the World Health Organization (WHO) to declare ” unregulated urbanization” as a communicable disease and include it in the ICD code sooner or later. (Air pollution is a masquerading term though!) .The urgency is real, since the apparent gain in life, due to modern medical therapeutics is getting rapidly eroded.
No more evidence is required to emphasize the fact, that enforced rural living is going to be an important CVD Intervention for the future. If someone (or any organization ) is still doing research to confirm this, please realize you are wasting time, stop it, and get on with corrective action along with the WHO’s other SDG goals.
Reference
Posted in Uncategorized |
Is it a STEMI or Non -STEMI ? The apparently realistic, but dichotomous thinking about ACS among physicians is existing for quite a long time. However, since the underlying pathobiology being same , it is worth wondering whether the conventional bifurcation of ACS is fool -proof , when applied to management decisions. The rapidity and totality of plaque fissure, rupture ,eruption,or erosion and the subsequent response of the local hemorheological system, determine the ferocity of the event.
How to recognise all these deep intracellular events in bed side ? Unfortunately, still with a lot of gratitude, we have to rely on the humble ECG for early segregation of ACS ,initiation of treatment. (Truthfully, Waller, Einthoven and Lewis should still be celebrated as forefathers of ACS )
Though STEMI/NSTEMI show different faces of ACS, however, it makes little logic to have two big set of guidelines when a patient presents with ER with resting angina with variable ST/T changes* .(In the very early hours of ACS, ie just moments after biological trigger who can predict which patient will enter what path and evolve into STEMI or NSTEMI)
* Typically, predicting the ECG-plaque interplay in Wellens’s syndrome ,De-winter or for that matter , in any biphasic precardial T wave sydromes can stretch our coronary acumen to its limits.

Now, ESC 2023 task force hasrealised this .To bring bettter judgment with a open mind ,decided to merge STEMI/NSTEMI into a single guideline , of-couse a with different treatment flow paths for these two entites.
I could take three key messages from this new guidelines.
1.STEMI guidelines are largely unchanged. There is still a major role for fibrinolysis, if you realistically think, and decide, you can’t reperfuse in the cath lab within 120 minutes after arrival.(120 mts time clock should start, much earlier is different debate!)
2.In NSTEMI, there has been important downgrading in the urgency of intervention even in the high risk category (Early invasive <24 hrs from class 1 to 2A)

3. Aspirin and regular unfractioned Heparin continue to rule the ACS world in most situations across the entire spectrum of ACS, except during the short peri-procedural period ,we need the assistance of new powerful P2Y12 blockers like Prasugrel or Ticagrelol.
Prof. Robert Byrne, from Ireland, succinctly explains the new ACS guidelines
Final message
Knowledge must be allowed to evolve, without any conditions or denials. Backtracking is an essential expertise, which can be as important as looking forward.
Posted in Uncategorized |
It was 2006
Allow me to recount an unassuming piece of a PowerPoint presentation from my institute, Madras Medical College, at the annual Cardiological Society meeting in New Delhi. The paper was categorized under miscellaneous sessions. I vividly remember the day. I have to admit, It was a nearly empty hall E, located in the basement of Hotel Ashoka. After the talk, I looked up to find that neither the chairman nor the handful of kind academic souls had any questions or comments to make. Pausing for a few moments, I quietly walked down the podium with an inexplicable silent pain.
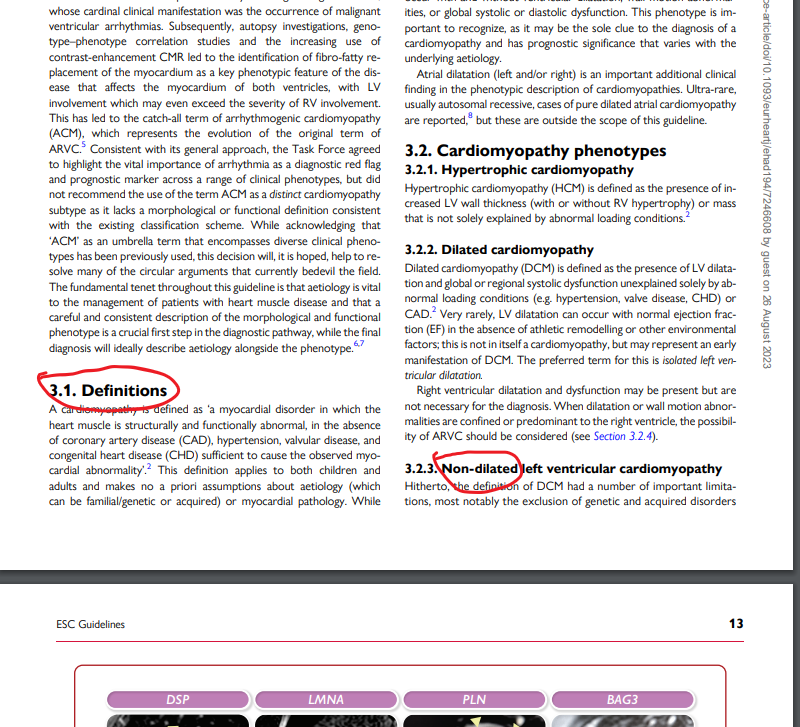
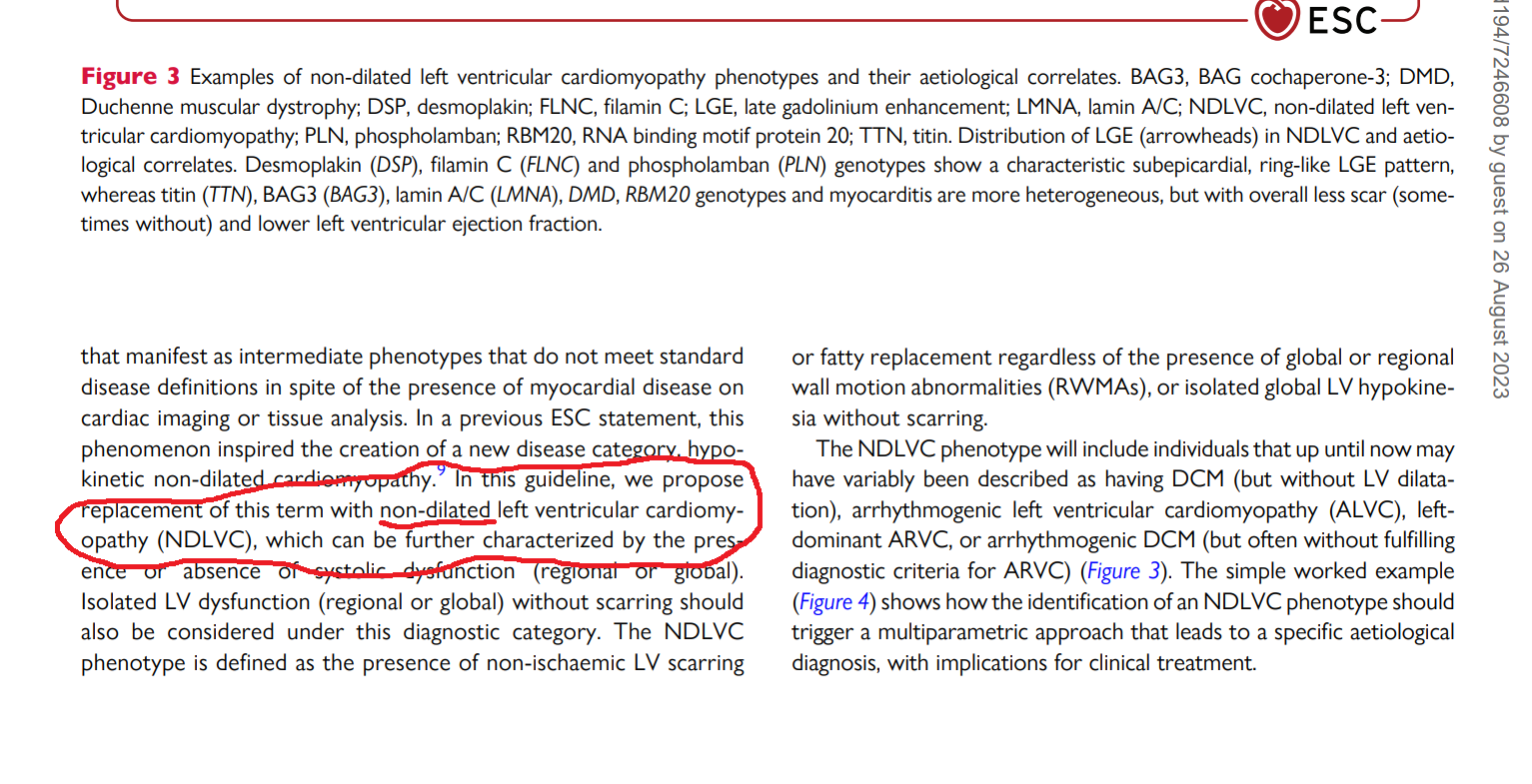
The title of the presentation was “Non-dilated cardiomyopathy”
Welcome to ESC Congress Amsterdam August 2023
ESC, has come out with this new update on cardiomyopathy. It is a pleasant surprise to find the term “Non dilated cardiomyopathy” entered the cardiology academia, authenticated by the ESC.
I must confess, it is difficult to conceal the joy and a little bit of self-pride.
Some observations from this document
1. Despite our tremendous knowledge base, we are yet to hang up our boots, in pursuit of an Ideal cardiomyopathy definition. Genotypic or phenotypic ? Phenotype is closer to reality, while genotype is largely imaginary. It looks like, The newer guidelines are moving towards a phenotype-based approach in all aspects except in risk prediction. Fair enough.
2. All cardiomyopathies, whatever way we segregate, ultimately end up in the common clinical syndrome of heart failure. So. it is better to spend some quality time here and concentrate on HF therapeutics.
3. Cardiologists are expected to critically fine-tune their general medical knowledge, which will help recognize and treat systemic disorders like Amyloidosis, and other metabolic infiltrates.
4..Almost all RCMs have non-dilated ventricles, so why a new term NDLVC? Anyone wants to ask this question ?. Further, there can be significant overlap between RCM & NDLVC as well. Definitely, there is a lot to understand beyond this 2023 document.
5. Why do some ventricles refuse to dilate even in the face of adverse hemodynamic and pathological conditions. Is it an advantage or disadvantage? If ventricles are adamantly stiff and decide not to dilate, there is no other option, the atria will proxy dilate, creating more problems in the lung circuits. This also raises a fundamental question Is NDCM a better stress buster (think Laplace law ) than DCM? or vive versa , the accomodative nature of LV passify & blunt the slope of LVEDP at times of exertion.
6. One more reality is, NDLVC is also an Important subset in the now fashionable HF entity HFpEF
Final message
The message to youngsters is this. Discuss, debate, and document your thoughts in whatever forum, that is available. Don’t wait for all those big brother journals and their recognition. If there is truth in your writing, someday it will be revealed to the world.
Reference
Posted in cardiomyopathy, Dilated cardiomyopathy, hypertrophic cardiomyopathy, ischemic cardiomyopathy, Uncategorized | Tagged drsvenkatesan, ESC 2023 new cardiomyopathy guideline, ndlvc, non dilated cardiomyopathy |
Lifestyle modifications and non-pharmacological modalities should be started in every hypertensive individual before starting them on long-term drugs. This is one of the foundational lessons in the therapy of hypertension. (Please mind, in no way, it conveys a meaning that we can give less importance to them after starting drugs.)
Exercise prescription has become a big-ticket event in hypertension clinics in recent times. Though any physical activity in adequate quantity is good, we have classified exercise into complex subtypes and found fancy ways of its administration.
Traditional belief gets a kick-back
We (At least me!) have been taught, isometric exercise is not BP-friendly. In fact, it can cause intermittent spikes that may persist for a variable duration depending upon the basal as well as dynamic adrenergic vascular tone. This is what I had taught to my students. This presumption is nearly shattered by this meta-analysis. It concludes that among all, Isometric exercise reduced the BP more than others. (especially wall squats and planks). More surprising is, that the usefulness of aerobics is lesser than dynamic resistance training as well.
Final message
Contrary to popular belief, Isometric exercise is not really hard on blood vessels and is likely to have a more favorable effect on blood pressure than aerobics.
Still, hesitating to fully accept the conclusion of this study. Exercise prescription is highly individualized & includes multiple cross-over strategies and self-learning. Caution is required when doing strong isometric exercises, especially after a vascular event.
Reference
Posted in Uncategorized |



