Cardiologists have always struggled to classify, assess, and grade one important valve disease, which is Mitral regurgitation. While valve replacement is the ultimate treatment, the timing of MVR is still a big debate. Apart from valve replacement, valve repair is a strong contender in selected patients. In recent times, cardiologists have made great strides to grab MR patients from cardaic surgeons. MitraClip, a percutaneous edge stitching , is possible with a varying degree of success.
Mitral valve edge-to-edge repair (MEER) is an interventional clone of Alfieri surgery that has shown conflicting results in the MITRA-FR and COAPT studies. The reason for this discrepancy in the MITRA-FR population is that they had larger-sized ventricles, which continued to pose challenges for the clip, which is focused only on the leaflets.
A new subdivision of secondary MR
Now, some of the cardiologists want to classify SMR/FMR into Proportionate vs Disproportionate MR. It may not be a great innovation, but it sub-divides secondary MR for optimal therapy. It simply says if LV dilation is significant, clipping the leaflet alone will not be sufficient; it would rather need an annular restriction either at the time of the index clip procedure or in due course. While Disproportionate MR implies, it is more of a leaflet coaptation defect, dominating over annular contribution.
Who proposed this ? What is the implication?
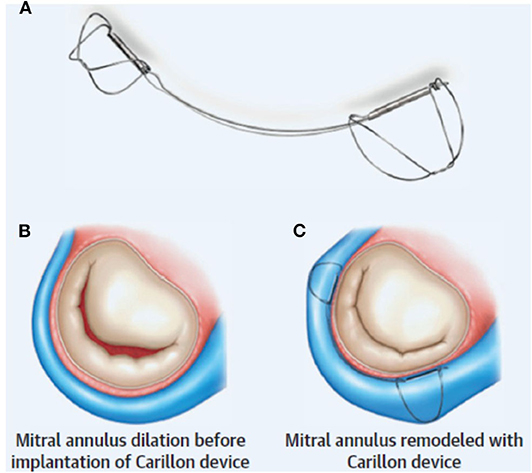
It is an afterthought, I think, from the makers of annular restriction device makers. MEER is found to be less effective in proportional MR.The Carillon device is a new arrival to tackle secondary MR .It is actually a wire that forcibly tightens the AV annulus inserted through coronary sinus . This modality takes advaantage of the aantomical proximity of coronary sinus to mitral annulus. Coronary sinus encircles and from a virtual wall along significant circumference of mitral annulus.
Unlike mitraclip, the Carillon device is claimed to tackle secondary MR irrespective of whether it is proportional or disproportional. It also has the potential to reduce LV dimensions in the long run. We have another device called IRIS-Millipede (to compete with Carillon).
Sec. Structural Interventional Cardiology
Volume 7 – 2020 | https://doi.org/10.3389/fcvm.2020.576058
Final message
We are free to have as many classifications in MR (Primary, Secondary, Functional, Atrial MR, & now Proportionate Disproportionate.) It is not the aim to bring up a rivalry between leaflet vs annular intervention. Ultimately, the most powerful component of the mitral valve apparatus, i.e., the LV muscle that matters.
I would request the esteemed researchers in MR ,not to keep EROs, regurgitation fractions, or chamber dimensions as primary markers of success of a device. Having strong clinical outcomes as the endpoint should be made mandatory, i.e., prolonging good quality of life and survival (But, the reality can bite hard. Someone told me, walking 20 meters extra in a 6-minute walk test is enough to get device approval from the authorizing entities.)
Final message
Postamble : A surgeons perspetive
While we debate about devices, the true benefits may lie elsewhere. A good MVR done by a mitral heart surgeon is the need of the hour. Says this paper from a top heart surgeon in India. Yadava OP. Disseminating valve repairs – a clarion call. Indian J Thorac Cardiovasc Surg. 2020 Jan;36



