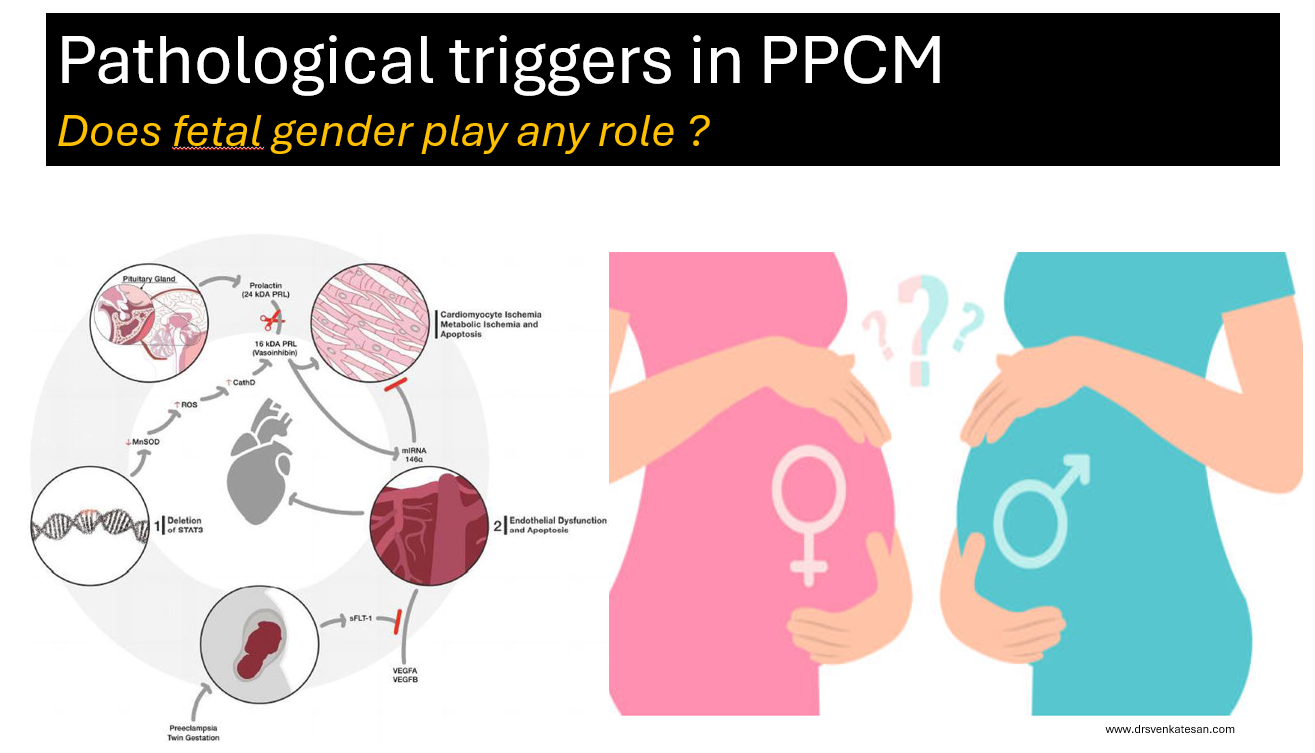
PPCM is a rare but an Important cardiac condition, that contribute to significant maternal and fetal morbidity and mortality.So many variables , triggers, back ground risks have been studied for decoding the pathogenesis of PPCM.
Does the sex of baby inside the mothers womb, in any way influence the incidence of PPCM ?
When searched in the literarure, I found almost no data on this simple parameter. While there is a lot of reference for PPCM relationships in twins and multigravida, none looked at gender specifically. From personal discussions with my Obstetrician colleagues, few suggested female babies are often seen to precipitate PPCM . I think it is an academic oversight, that we haven’t looked at the gender angle as yet, for this important entity.
Is there really no evidence ?
Yes, it is sursprisngly true . Gender as a variable may have been overlooked because it hasn’t shown up as a signal in preliminary data . Researchers often rely on patterns in existing data to guide hypotheses, and if no pattern suggests fetal gender matters, it may not be pursued. In some studies, gender data might be collected but not analyzed or reported.
It is a fertile research field. It may look like a simple study, but it can throw more light on this mystery myocardial disease that is directly related to pregnancy.
Could Fetal Gender Be Relevant in PPCM ?
While no evidence currently supports a link, there are theoretical reasons why fetal gender could be important.
Placental Differences: We know male and female fetuses have slightly different placental gene expression and responses to maternal stress, which could theoretically influence maternal cardiovascular load or immune responses.
Microchimerism: If fetal cells contribute to PPCM via immune mechanisms, sex-specific differences in cell behavior (e.g., Y-chromosome-related antigens) could be explored.( though this is speculative)
Hormonal Influence: Fetal sex might influence maternal hormonal profiles (e.g., via placental hormones), Female fetus are known to have more intense estrogenic effect in maternal circualtion.
Pregnancies with female fetuses may be associated with slightly higher levels of hCG or placental aromatase activity, which could theoretically enhance estrogen production or mimic an estrogenic effect in some contexts.(Ref 3)
What are the maternal diseases that are shown to be correlated with fetal sex ? (Ref 1, & 2)
Some maternal diseases, such as preeclampsia, gestational diabetes, preterm birth, hyperemesis gravidarum, autoimmune diseases, and asthma, have been associated with fetal gender in limited studies, with male fetuses often linked to slightly higher risks for preeclampsia and GDM, and female fetuses to hyperemesis and asthma exacerbations. However, these correlations are generally weak, and mechanisms are not fully understood. For PPCM, no evidence exists
Final message
Fetal gender is a simple, routinely collected variable, making it feasible to include in future studies without significant cost. If even a small association exists, it could refine risk stratification or guide mechanistic research (e.g., exploring sex-specific placental factors). The lack of data on this parameter represents a knowledge deficit in cardio obsterics that could be addressed in large registries or meta-analyses, especially as PPCM research has grown significantly in recent times.
*Request the fellows in O&G and cardiology to conduct a specific study on this topic and enrich the literature on PPCM. I think the data is already there in every PPCM paper. We just need to collate. (There is no copyright for this topic, but please acknowledge, if no one has done this aspect of a study in PPCM before)
Reference






