Doctor, should I restrict sodium , if so how much ? one of my patient with heart failure asked ?
*Cardiac failure is a condition where RASS is activated , kidneys become salt & water avid”
A recent Viewpoint in JAMA Cardiology titled “The Sodium Paradox in Decompensated Heart Failure” challenges the longstanding practice of strict sodium restriction in heart failure (Ref 1) While traditional management assumes that limiting sodium intake counters the sodium-avid state and promotes decongestion, emerging physiological and clinical data suggest that overly restrictive sodium diets may paradoxically impair effective diuresis in some patients. This may occur through activation of compensatory neurohormonal mechanisms or by blunting the natriuretic response to loop diuretics. The authors advocate for a more nuanced and individualized approach to sodium intake during acute decongestion, potentially including controlled sodium supplementation in selected cases.
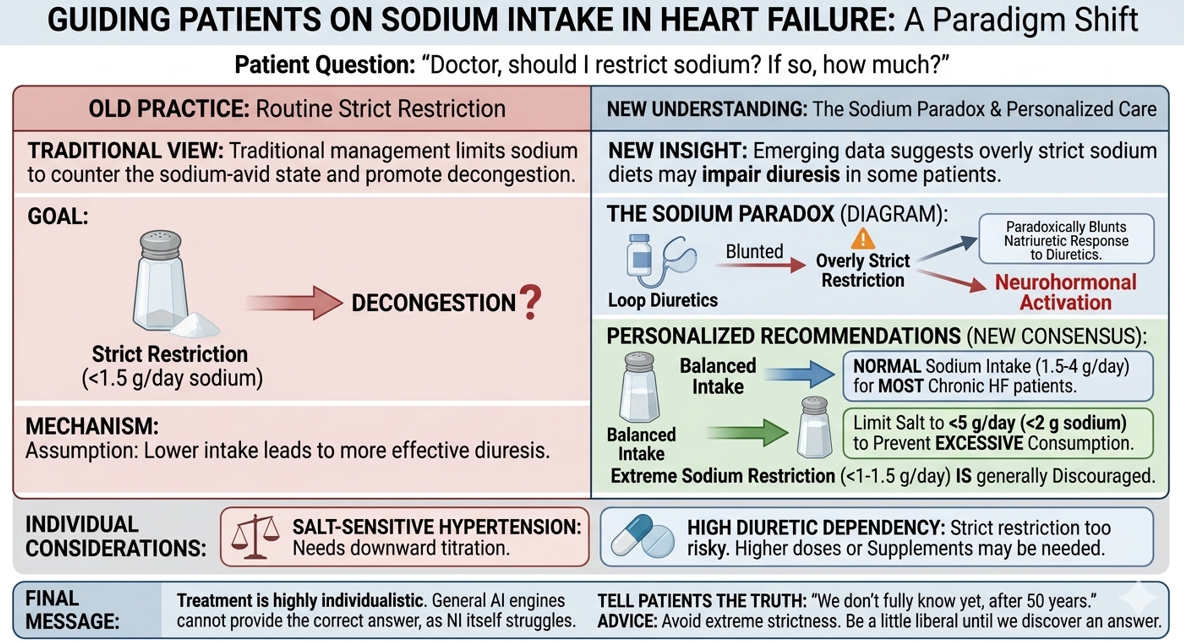
This is consistent with the 2024 Heart Failure Association (HFA) of the ESC clinical consensus statement on dietary sodium and fluid intake in heart failure.(Ref 2) The statement highlights that recent randomized evidence has weakened support for routine strict sodium and fluid restriction. It recommends limiting salt intake to no more than 5 g/day (2 g sodium) in patients with heart failure to prevent excessive consumption, while endorsing a normal sodium intake (1.5–4 g sodium/day, equivalent to up to 5 g salt) for most patients with chronic HF. Extreme sodium restriction (<1–1.5 g sodium/day) is generally discouraged as it may be counterproductive. Please mind,fFluid restriction (1.5–2 L/day) is also reserved only for selected patients, such as those with severe hyponatremia or refractory congestion.
Other considerations
If a patient relies on a high dose of diuretics, limiting salt can be risky; they may actually need more supplements. Contrary to popular belief, more than loop diuretics, thiazides, especially metolazone, can lead to more sodium loss.We used worry more about hypokalemia with diuretics, now only we realised sodium loss is equally important. If the patient has salt-sensitive hypertension, the salt should be more carefully prescribed. Even mild impairment in kidney function can further complicate alter the sodium metabolism*. Ultimately, treatment must be tailored to the individual, and no AI can provide a definitive answer, as even medical professionals face. challenges in this area.
Final message
So, when the next time your patient asks you, “Doctor, should I take less salt?” please be truthful and tell them we don’t know the exact answer to this simple question yet, even after 50 years of cardiac research. However, we do know , need not be overly strict with salt control, be a little liberal until we find an answer.
References
- Testani JM, Mullens W, et al. The Sodium Paradox in Decompensated Heart Failure. JAMA Cardiol. Published online April 29, 2026. doi:10.1001/jamacardio.2026.
- Mullens W, Damman K, Dhont S, et al. Dietary sodium and fluid intake in heart failure. A clinical consensus statement of the Heart Failure Association of the ESC. Eur J Heart Fail. 2024;26(4):730-741. doi:10.1002/ejhf.3244
Postamble
*Can we get an answer from a Nephrologist ?
I asked my colleague, a Nephrologist, about salt restriction in heart failure. Our discussion revolved around pre-renal states, glomerular physiology, sodium natriuresis, free water excretion, etc. I asked him, is water or sodium real enemy of kidney during circularory distress ? He wasn’t sure . I was not sure about the same in cardiac failure .In the end, it became too complex for both if us.
It seemed obvious, how widely our two specialties have separated, even though they deal with the same human circulation. The irony is, these two organs (heart and kidneys) are just half a feet apart in our body.



