PH has always been an exciting academic topic in cardio-pulmonary medicine, for both clinicians and researchers. It is also one of the extensively studied hemodynamic parameter. The pressure in pulmonary circulation is intimately tied to the function of two critical organs. lungs , heart and various systemic factors. The fact that pulmonary circulation is essentially expansive & engulfed by the dynamics of lungs, makes PA pressure a continually variable parameter. Further ,the chest wall compliance, airway resistance , influence of pleural pressure fluctuations, make it difficult to estimate the normative pulmonary artery pressure and resistance even in rest.(Imagine during exercise !)
No surprise, our knowledge base about PH is under constant flux. The trouble starts with this query, What is the normal PA pressure ? After toying with various numbers we are currently hanging all our wisdom at a mean PA pressure > 20 mmhg as cut-off to define PH. However, we are able to grossly classify PH into various categories , pre/ post /combined etc. Here again, we have a guess work with two more cut offs.. For PCWP we have decided to choose 15mmhg over 12mmhg as upper limit of normal & PVR < 2 Wood units.
The second query in PH is still more contentious. What is the effect of exercise on PA pressure ? In our student days we were not allowed to bring exercise into the picture of pulmonary hypertension, in spite of the fact cardiac output increases up to 5 fold during peak exercise, Now, there is evidence to show exercise can increase PA pressure significantly, beyond the limits of current definition of PH. This is problematic for obvious reasons. Still, there has been considerable reluctance to accept exercise induced PH as a clinical problem by many of us .
*To be fair with our intellect, I think, we haven’t yet approved “Exercise induced systemic HT” as an entity officially. (Of course, hypertensive response during stress test is well known)
Seeds of New thinking
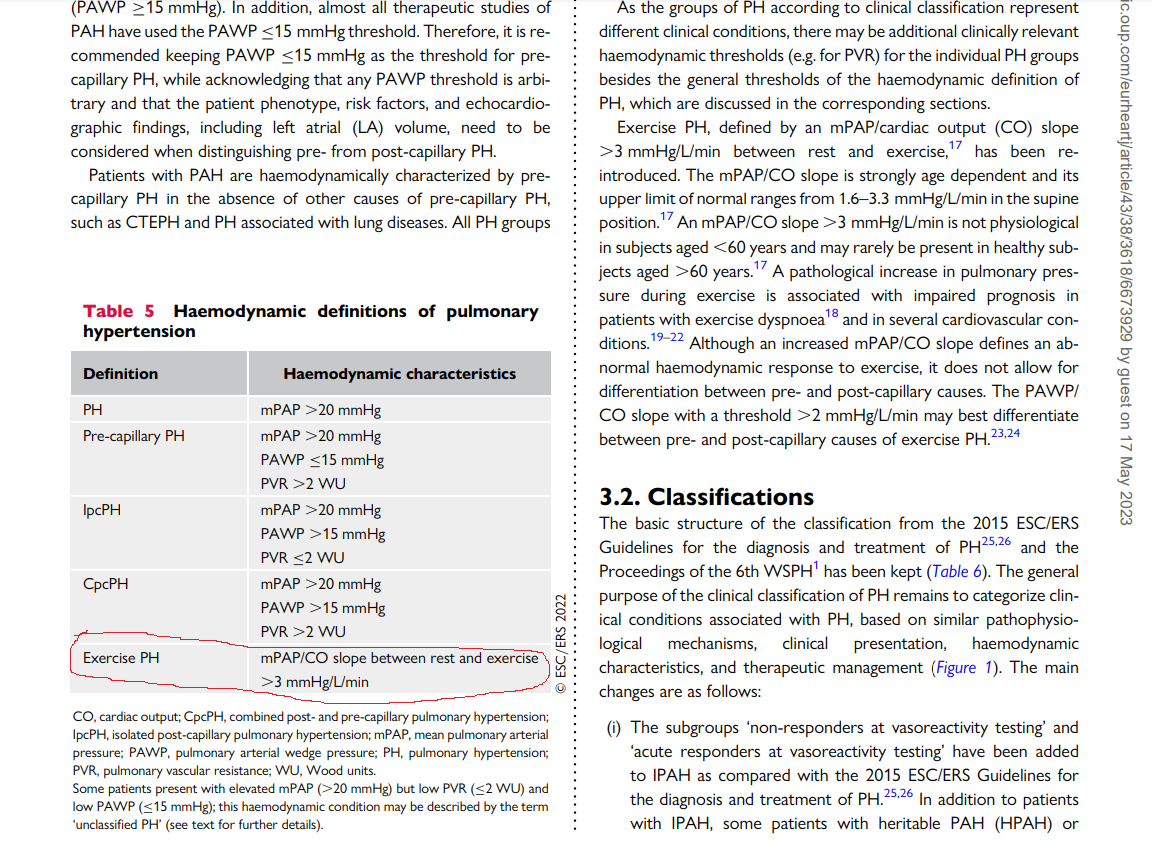
Thanks to current guidelines from ESC in 2022 .The exercise induced PH has come back with a bang and finds a place right behind the pre and post capillary PH. (See below ) I am sure, there must have been a vigorous debate before including this in the definition. We must appreciate the authors of two forgotten papers for the major shift in our understanding .(Ref 1 ,2)
The secret of the slope : From where did it come ?
ePH is > 3mmhg /Litter/Minute is the definition of ePH
Some questions on ePH
1.How do you define ePH ?
Mind you, it is not an absolute number. It is the slope more than 3mmhg per litre of cardiac output. I agree to measure the slope > 3mmhg we need serial measurement and may be impractical .(Immediate post exercise echo is a close alternate )
2.Why we depend on slope rather than absolute value ?
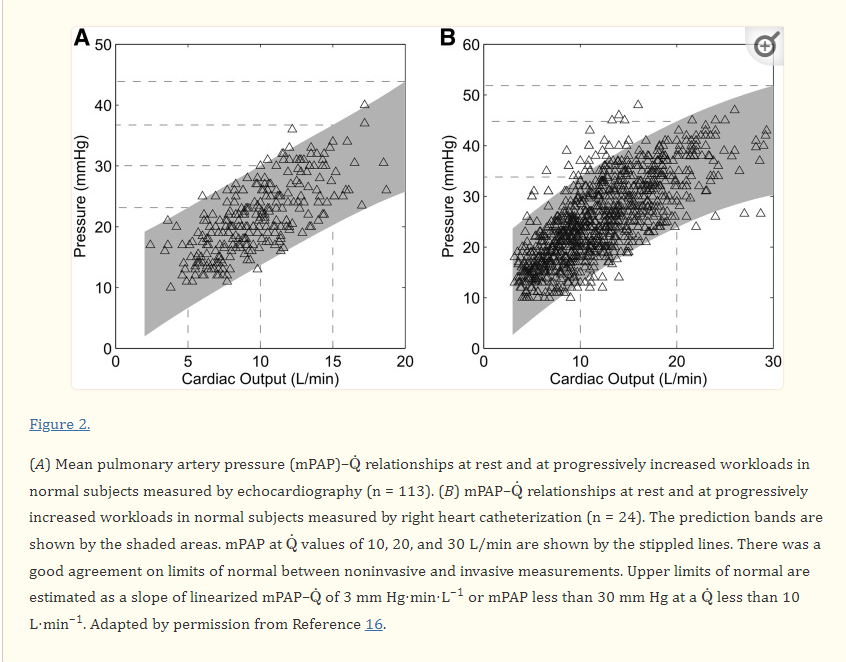
This is because during heavy exercise PA pressure can raise even up to 30 or 40 crossing the boundaries of PH ..Only the rate of raise ie the slope can tell us whether it is appropriate or inappropriate.
3.Does ePH is really a clinical problem ?
Yes. it should be suspected in every unexplained dyspnea .(Beware of the anxiety it may elicit to the patient, so, go slow with your investigation first rule is to rule out Anemia and other common causes )
4.Can ePH occur over and above established causes of PH ?
Why not ? it is very well possible.(PH before and after six minute walk test will unmask this component)
5.Can we further classify ePH ? (Pre vs Post cap ePH)
Possible yes. ePH can be a marker of HFpEF if LVEDP is also correspondingly increased or else it will fall in to CETP or COPD.
6.Can COPD cause ePH ?
Yes, possible.
7.How does RV function confound ePH ?
This is ticky. Perfect RV-PA coupling and a good RV function is required to sustain ePH. A poorly contracting RV will make the whole concept of ePH and the defining criteria redundant. May be, we need to work for RV function corrected ePH . (This is a potential research topic for fellows)
8.Where do diastolic stress testing fit in diagnosing ePH ?
In one aspect ,DST which is screening test for silent HFpEF is an example for subtype of ePH.
Final message
The concept of ePH has entered once again into the cardio pulmonary clinical domain. Thanks to ESC 2002 team for listing this hitherto ignored disorder. Let us reiterate the importance of this concept in the clinical practice. It is worth considering some form of stress test to recognise this entity, in every patient who has unexplained dyspnoea.
Reference
2.Bossone E, D’Andrea A, D’Alto M, Citro R, Argiento P, Ferrara F, Cittadini A, Rubenfire M, Naeije R. Echocardiography in pulmonary arterial hypertension: from diagnosis to prognosis. J Am Soc Echocardiogr 26:1–14. [PubMed]
Further reading
ESC 2016 guidelines on PH ;It is worth comparing he current guidelines with the last one published in 2016
European Heart Journal, Volume 37, Issue 1, 1 January 2016, Pages 67–119, https://doi.org/10.1093/eurheartj/ehv317



