Fibrillation is a continuous, chaotic muscular activity. In AF, atrial muscle is expected to lose all coordinated contractions with fibrillatory waves replacing P waves. Have you ever spotted a suspicious P wave in a strip of otherwise explicit AF? If not, this write-up is not for you.
An evolving rare theme in Atrial fibrillation
Have a look at this ECG
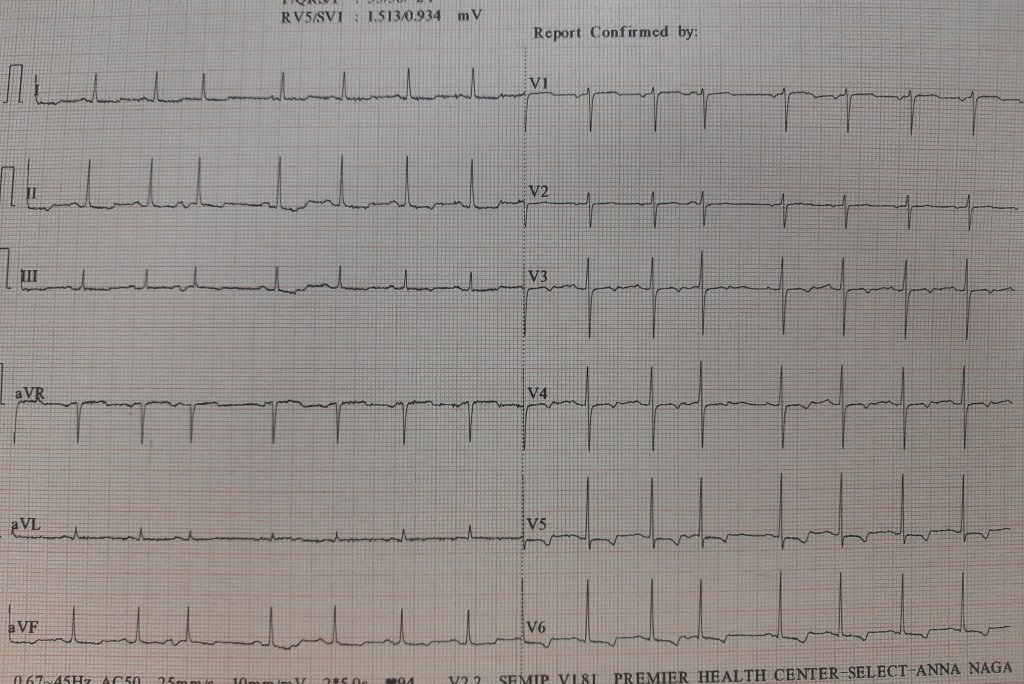
Here is an ECG, that was reported as AF, multiple APDs, or Possible AF, Pre AF. I suggested the term AF in transition. While few agreed, many said it is a straightforward SR with APDs, making it appear irregular RR.
But, the fact of the matter is, ECGs are insensitive to pick all fibrillatory wavelets. It can selectively pick a few coarse F waves and make them appear as P. I think, in this era, we should not diagnose AF by proxy, ie absent P waves. Rather, we need to look actively for fibrillatory wavelets. (Imagine all sinus arrests will qualify for f fine AF with a slow ventricular rate is it not ?)
The semantics of AF nomenclature is long. Intermittent AF, and paroxysmal AF, are well-known entities. It is now clear, AF can occur for a few seconds and vanish too. It seems we need to play some more linguistics with the most common cardiac arrhythmia. (Non-sustained AF, evanescent AF, etc )
Some thoughts on this hide & seek P waves
- Apart from the conventional list of absent P waves, one more example is repetitive APD can stun the atrial muscle for a few moments or minutes.
- Then, we always have the issue( eluded to earlier) of sinus node paralysis, with irregular junctional escape mimicking AF.
- Amiodarone can reduce fibrillatory rate, and (AF cycle length ?) Coarse F waves slow and stabilize it to mimic an organized P wave
- P on Ta waves (Like R on T ) can trigger a nonsustained AF for a few moments in a functional manner without real pathology in atria.
A funny memory brings back an EP truth
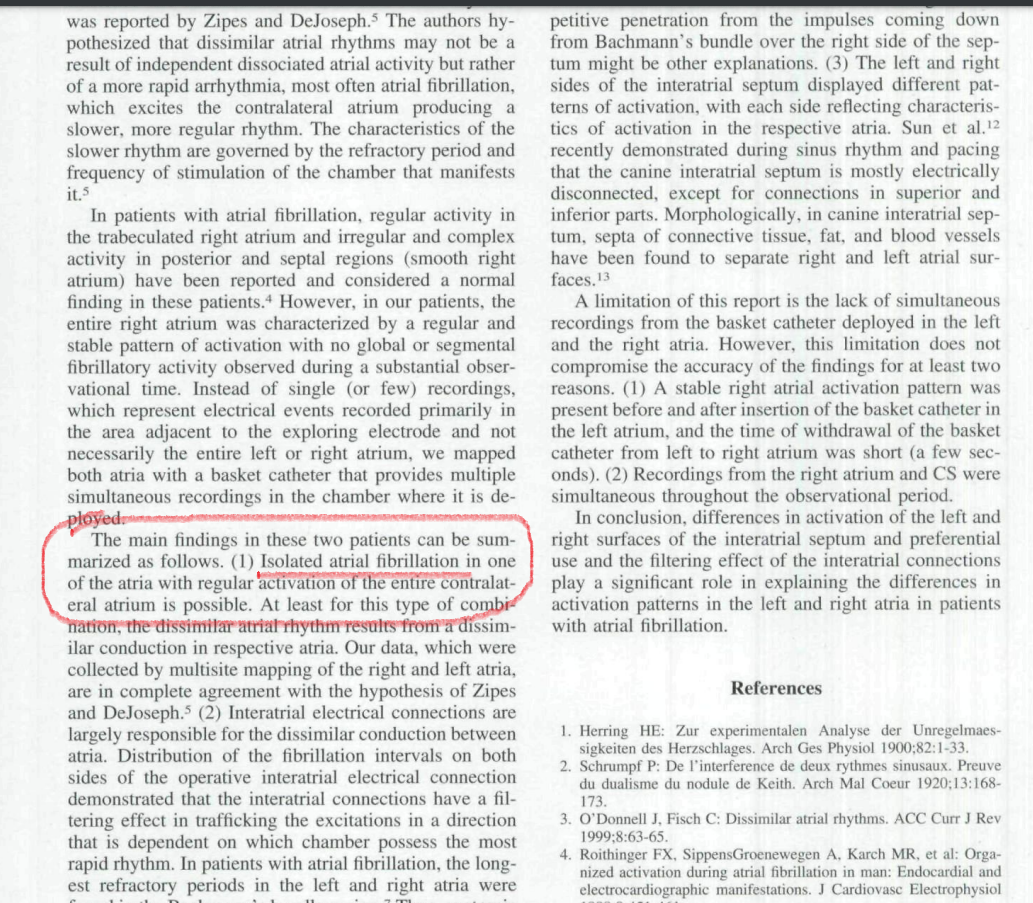
During our student days, my Professor used to trap us with this question, Which atria would fibrillate in mitral stenosis? Many of us blinked, and few had no hesitation to say, it is the LA that fibrillates. Now, after 50 years we realize, how fascinating the secrets AF has unfolded. Some organized activities are often in the right atrium, even as LA begins the process of AF. It is possible it may take variable time for the left atrial chaos to spill over to RA*. During these electrical uncertain times, some of the right atrial P wave activity refuses to die down. Even more dramatic one Atrium alone can permanently fibrillate and others completely insulated by blocking the signal in the Interatrial pathways. (Ref 1 ) Ndrepepa’s paper in the JCE 2000)
Final message.
True scientists rarely bother about questioning a dictum. The concept of non-uniform AF was first thought of by (Schrmp et al Ref 2) 100 years ago in 1920, and Zipes(Ref 3) hypothesized this in 1973. now, in the Year 2000, Ndrepepa confirmed it with EP studies. The spotting of occasional P waves is not forbidden in AF if the contralateral atria decide to block the incoming AF signals and keep generating their own P waves
Young EP guys, now that you are equipped with the sophisticated intracardiac GPS, please pursue this provocation in AF. One more piece of evidence we observed in the echo lab. Try to look at Tricuspid doppler A velocity waves in full-blown AF patients. You can see the surprise for yourself. This is very good research work to do. This is one of the ideas I gave to my fellows at MMC. Now, it is free for all to pursue whoever wants to do this. The clinical implication* will follow.
* A lingering query, how common is RAA clot in mitral stenosis with AF and the possible threat of pulmonary embolism?
Reference
2.Zipes DP. DeJoseph RL: Dissimilar atrial rhythms in man and dog. AmJCardioi I973;32:6l8-628.
3.Schrumpf P: De 1’interference de deux rythmes sinusaux. Preuve du dualisme du nodule de Keilh. Arch Mai Qwur 1920;l3:168-173
Postamble
The snapshot from Ref 1 . The term Isolated AF confined to one atrium could be a rare event, but, no one can deny we have plenty to learn from them