The main reason for all those jitters, we cardiologists, get every time we puncture the IAS is not due to a lack of expertise and experience perse. There are two more reasons. First and foremost, it is still largely a blind* procedure. (Even in this era, where drones with HD vision shoot one-meter targets from a 1000 KM range ) *TEE and ICE are there, but they rarely give enough confidence.
The second reason is more important and is rectifiable. It is the perception error in our anatomical cognition, that is fed to us from first-year medical school. We are made to believe (at least to people like me ) The right atrium is aligned like a perfect box on the right side, sharing a wall called IAS, and the left atrium is obediently placed left of the right atrium. Please realize the heart is such a complex twisted single tubular organ, the venous end, in a stunning backward loop brings the LA most superior and posterior to the right atrium overriding the left-right relationship.)
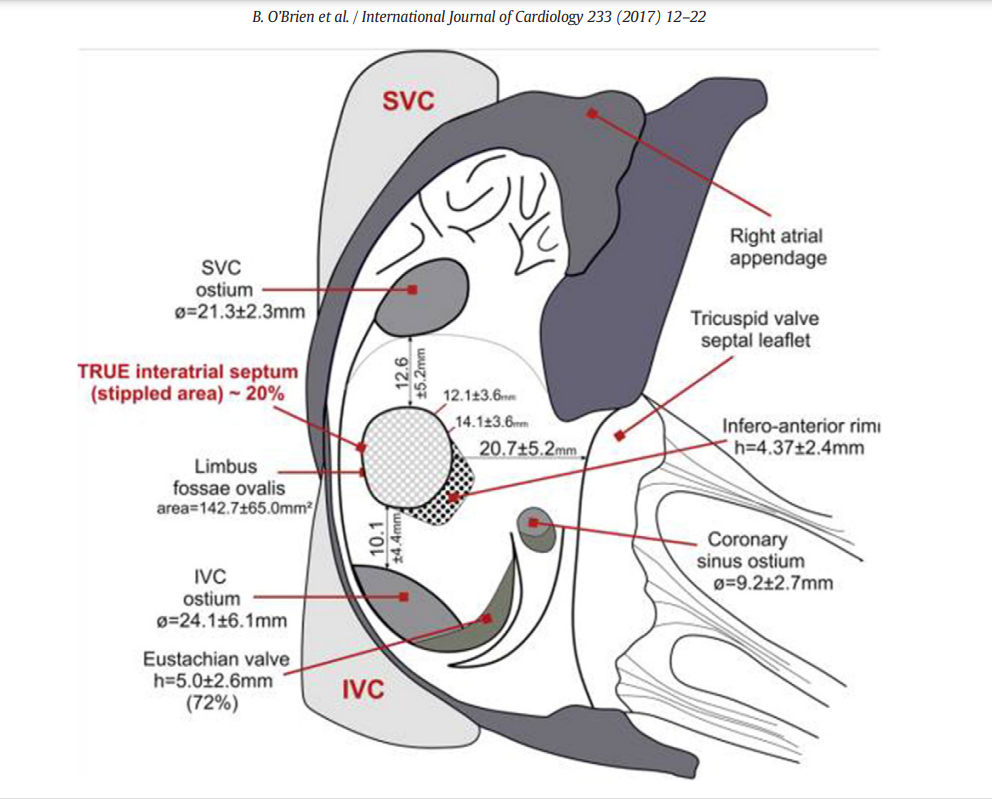
The right atrial terrain and IAS with multiple bumps and holes. Note the true IAS constitutes only 20% . This is where our punctures need to be.
Development of IAS
IAS development and the number of layers it sandwiches, the tortuous tracts of PFOs, the fossas, and its variable limbus is a big topic. Further, It is worth recalling, the true IAS hardly forms 20 % of the area of the interatrial contact surface.
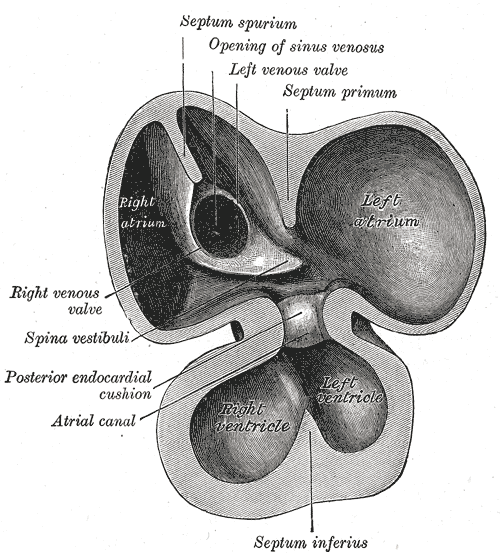
(the differential regression of sinus venous, along with infolding of the roof and along with curious septum spurium , the ubiquitous septum secundum make the texture, area & shape of IAS, a fascinating creation, though troublesome for the cardiologists ! ) Whoever named that part of vanishing IAS as spurious, (I think it is Henrry Grey ) has much fore-vision.
Forget about all this. Tell me how to cross this difficult terrain
Coming to the real world of interventions, we need to do targeted punctures in different spots of IAS in various interventions.(Mitra clips, LAA device, PTMC, PV abaltions, Mitral paravalvular leaks , TMVR etc) This has made this task even more tricky. Experts are always there to help us out. Like swimming, it can never be learned in books.
This 19-minute clip from. Seoul, South Korea is an excellent resource. Thanks to Dr. Sang Weon Park
Along with sound anatomical knowledge, improved hardware, and imaging like deflectable sheaths, TEEs, and ICE (intracardiac echo ), let us hope, it will soon become an easier task for everyone.
Final message
Understanding “attitudinal cardiac anatomy” with fluoroscopic overlay is the key. Again, it needs to be stressed, “Right is not right, and left is not left” when it comes to true atrial geo position. LA is equally posterior, superior, and of course to the left of RA. Some of my colleagues are blessed with a special 3-dimensional skillset (Inherited ?) I failed miserably to understand this, till very late. I am sure, Dr. Park’s video will help all our youngsters to cross the difficult gateway to the left side of the heart.
Reference
One more good read
B. O’Brien et al. / International Journal of Cardiology 233 (2017) 12–22



