Once the Noble and pride profession, practicing medicine is becoming fearsome. India’s healthcare system is facing a silent emergency, not of disease, but of distrust. A worrying wave of rising intolerance among patients has led to an alarming surge in verbal abuse, threats, and physical assaults on doctors. Once revered as lifesavers, doctors now work under the looming shadow of mob rage, fueled by unrealistic expectations and social media-triggered misinformation. Emergency rooms have become battlegrounds. This is not just a law and order crisis—it is a near collapse of the doctor-patient relationship, once sacred, now strained to the breaking point. Urgent systemic, legal, and cultural interventions are no longer optional they are are matter of survival.
While the issue looks monstrous, if we dwell a little deeper, it is clear case of miscommunication, over-expectations, low tolerance, and sheer ignorance about human biology and illness . With the destructive mass of information explosion , every patient tries to think more than a doctor, about his or her illness.
This curious thought popped up during a debate with my colleagues . Why not propose a Hippocratic-like oath for every patient and their close family members as they enter any public or private hospital .Hippocrates would have never Imagined , there would be need for such an oath from patients.
Here is the Hippocratic Oath : Patient version 2025 : *Disclaimer : The content is never meant to underestimate the freedom and rights of the patients. While the patients are becoming hyper educated , with various resources , this oath is an attempt to enlighten them some simple but Invisible truths in our profession.
I am sure, this might look harsh, provocative, and even belittling of patient rights. But, to my conscience, it looks like, we the doctors have failed the whole patient population, by behaving, as if we are doing the job of a God. (at least in India) In the process, we have hidden many errors and systemic malfunction that are built into the system. We hesitate to tell the truth .For example . the true medical risk is dynamic and can vary moment to moment, even with an apparently simple procedure. (1% risk can become 100% risk in a flash ( A minor lapse of concentration* during a complex surgery or procedure can lead to… )
No surprise, patients expect 0% error and 100% success. Think for a minute and reflect. When did you last admit to your patient, “Yes, it was a mistake or error on my part?” That’s where the seeds of problems germinate. In spite of the dedication (& sacrifice) of our entire lifetime to our patients, we stand sorry. We must ensure and sensitize our patients, that complications and errors are irreversible attachments of disease and the treatment process. (As of now, so called informed consent document in India, doesn’t even receive the respect of torn rubbish in the dustbin.)
*Full time sports professionals like Messi or Ronaldo can miss a penalty kick in a most crazy fashion, Virat Kholi can see his middle stump flying on the first ball, but Doctors can never err* … they need to be perennially precise, 24/7 X 365 .How fair it is ? Wish, God shall answer this query for our beloved patients.
** But, the truth is , they err quite often is the untold story .The day our beloved patients realize this, medical profession will be released from the clutches of distrust from the patients.
An Awakening Call to the Guardians of Medical Science
Dr. Venkatesan Sangareddi MD, Former professor of cardiology, Madras medical college,Chennai .India
Medical science remains a cornerstone of human progress, and what we have achieved in the last 100 years is unprecedented. Every one of us is aware that the trust placed in medical research is sacred. Also, the medical profession is expected to remain noble as long as human beings exist. However, as in all walks of life, there must be trade-offs to any positives. Yes, this trust has increasingly become vulnerable, threatened by the pervasive and often subtle influence of conflicts of interest (COI). This is especially explicit in the current medical research landscape.
While the scientific community has made strides in acknowledging and requiring disclosure of COIs, particularly from authors , the measures are proving insufficient. There is a big irony sitting right across us. It is made to look, as if conflicts of Interest (COI) exist only with the authors.
The following article written by the author (Ref 1) calls for an awakening to every medical journal publishers, regardless of their prestige or impact factor, to recognize their vulnerability . We are expected to adopt a new paradigm of transparency in declaring COI, that extends to every participant in the publication process, including the scientific or ethical committies that approve the study ,the peer reviewers, the publishers and finally to the industries that fund the research.
Reference
1,Click here to download the full paper:A caution: It is a fairly lengthy article. (15 minutes read) Hope the suggestions made in the article are not labeled as unrealistic and possibly crazy as well.
Measurement of pulmonary vascular resistance (PVR) is traditionally done by cardiac catheterization. It remains the (un)disputed gold standard, despite numerous assumptions, errors in measurement, and lack of reproducibility.
PVR by Echocardiography
Recently, echocardiographic calculation of PVR gained importance. Resistance is pressure divided by flow. Pressure is measured by Doppler, flow is measured by the cross-sectional area of RVOT times the TVI. We can arrive at PVR quickly. As simple as that.
Still, many institutions and purists ( Who have huge trust in cath derived, Oxygen diluted data) ) won’t accept this as standard . They fail to realise echo methodology carries less limitation, if not similar limitations as in traditional cath method. However, a significant advantage is, it is more real -time, can be repeated any number of times, and documents a baseline PVR, and at least is useful for follow-up.
There are two formulas used.
1.Abbas Formula
PVR = (TRV / RVOT VTI) × 10 + 0.16
2.Haddad formula :
PVR= (TRV²/VTI_RVOT)
*TRV = Tricuspid Regurgitation Velocity (m/s)
*RVOT VTI = Right Ventricular Outflow Tract Velocity Time Integral (cm)
Comparing Abbas vs Haddad
The Abbas formula is better validated and widely used in clinical practice, as it was specifically designed to correlate with catheter-based pulmonary vascular resistance measurements. It provides reasonably accurate estimates, especially for screening pulmonary hypertension, though it tends to under-estimate PVR at higher values (>8–10 Wood units).
In contrast, the Haddad formula ) is simpler but less rigorously validated and is more commonly applied in research settings focused on right ventricular-pulmonary artery coupling rather than direct PVR estimation.
Haddad’s method may be less reliable in patients with significant tricuspid or pulmonary valve abnormalities. Therefore, Abbas remains the preferred formula for routine clinical application. There is still hope to improve Haddad equation.
How to improve upon Haddad equation* ?
The Haddad equation for estimating PVR (TRV²/RVOT VTI) lacks calibration and overlooks key hemodynamic variables. It can be improved by introducing empirically derived correction factors to correlate with catheter-based values. Incorporating right atrial pressure (RAP), RV functional indices like TAPSE or RV strain, and adjusting for heart rate or rhythm variability can enhance accuracy. Averaging VTI across multiple cardiac cycles could also stabilize measurements. Additionally, machine learning on large datasets and AI-enhanced model could outperform the current linear Haddad formula for non-invasive PVR estimation.
* This is a fresh area of study , young fellows should come forward to do.
Final message
As discussed earlier, Abbas remains the preferred formula.But, the real issue is cardiologists refusing to accept any Echo-derived PVR and incorporate it, in the day to day practice. We have accepted EF % as the gold standard for LV function in spite of some serious lacunae. PVR carries the same story. Cath-derived data, in all likelihood, is enjoying pseudo-sanctity. It is time we should embrace one of these Echo formulas regularly and make life simple for both ourselves and the patients (who are often tiny babies or children). I think it can be done without compromise on scientific purity.
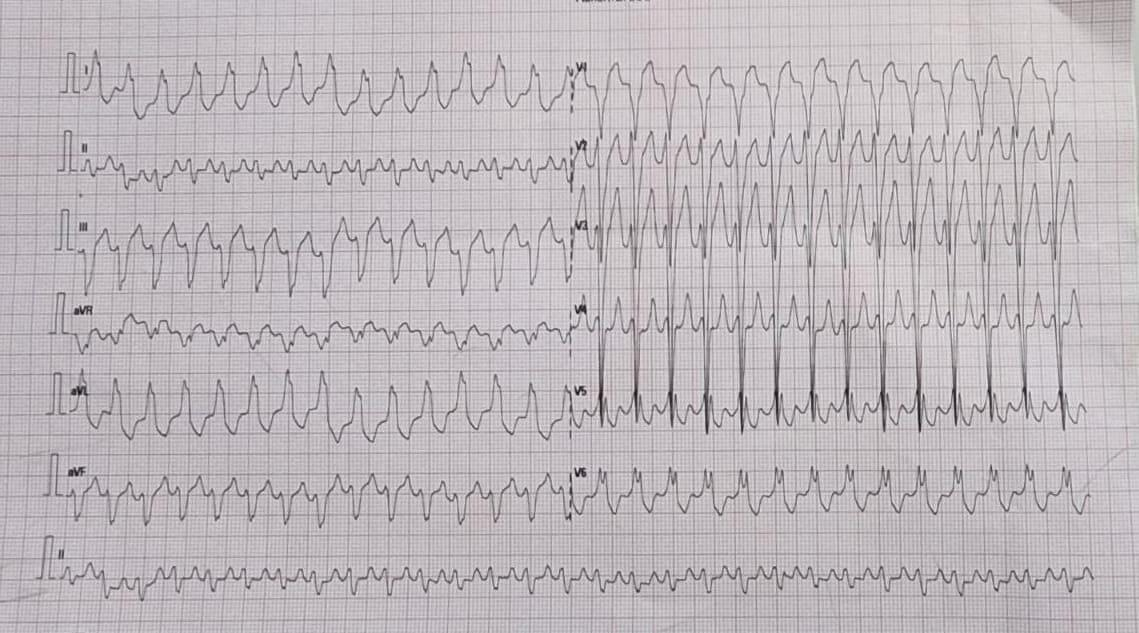
None exposes the expertise and stretches the electrophysiological acumen of a cardiologist, more than a strip of wide QRS tachycardia. Here is a patient who comes with palpitations, with mild hypotension , still comfortably entering the OPD with a non-emergency appointment.
How many diagnosis are running through your mind when you see this ECG . How much it got narrowed after applying criteria like Brugada, Vereckei etc ( VT, FT, OTVT, Mahaim Tachycardia, AVRT /AVNRT with aberrancy etc)
Now let me reveal the age of the patient .He is a 13 year old boy. Does this help you to narrow down the list of possibilities ? Logically, It should , but for some it can widen the list as well .( Brugada, Anderson, Long QT, Naxos all runs through the mind)
What happed next ?
As the cardiologist was wondering how to tackle this arrhythmia . Adenosine? Amiodarone or DC shock, thankfully, the boy got to spontaneous sinus rhythm .
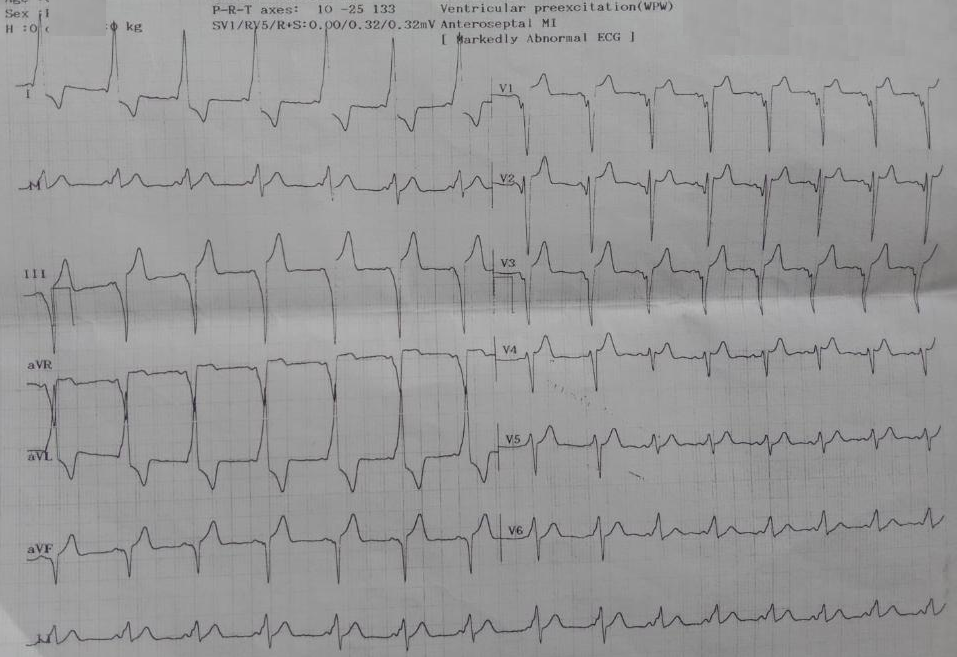
Yes it is a WPW substrate. Localization of pathway is a must and a headache for the fellows. .For me, It looks like a posterior pathway in the para-spetal area. 90% of AVRT are narrow QRS . Here it is wide. Why ?
It’s simple. The tachycardia is anti-dromic.
Is it ? Look at the strip again and confirm is this antidromic ?
I am not sure , I still think it is still antidromic .
I am saying No. This is Ortho-dromic wide QRS tachycardia .
How do you say so ?
Antidromic will still more wide and rapid and won’t terminate spontaneously .Of course one problem here aberrancy usually take an RBBB morphology.
How are you so sure . Let us send this to an EP guy.
*What did the EP say? Well, he didn’t commit to anything as I expected. He said until he measures the refractory period of the accessory path, he won’t comment anything about ortho or antidromic query of AVRT. He asked us to send the case for ablation immediately,
Ok. Let us analyse the reason for orthodromic wide QRS AVRT
1.Rate dependent aberrancy
2.Functional abberancy.
3.Preexisting BBB
4.If patients are on drugs that can prolong his Purkinje conduction
Final message
Two lessons may be learnt.
Lesson 1: Trying to decode a wide QRS tachycardia, without knowing clinical background, should be forbidden. This topic is intentionally made complicated by a flawed teaching methodology of wide QRS tachycardia for over 4 decades. Maybe the single lead AVR algorithm promises to be a quick remedy. If AVR is positive, it is VT; cannot be SVT.
(For the curious readers , please go through Dr. Masood Akhtar’s article from Wisconsin on how to differentiate VT & SVT without even looking at the ECG by law of statistics that beat the invasive EP studies).
Lesson 2 : Wide QRS AVRT is not always antidromic . In fact, orthodromic wide QRS AVRT is 2 to 3 times more common. Many of us don’t realise this bias in our learning.
In a country fighting hard to lower its maternal mortality ratio (MMR), one might imagine a clear cut focus on fundamentals like anemia, hemorrhage, sepsis, obstructed labor. But instead, a new fad has crept into antenatal care, camouflaged as progressive medicine. It is the routine ordering of maternal echocardiograms in all pregnant women, a trend that appears to be driven less by evidence and more by fear, peer pressure, and the increasingly fashionable distrust of clinical acumen.
Pregnancy is not a cardiac disease. In fact, most young Indian women undergoing childbirth are remarkably resilient physiologically. But, thanks to a few well-publicized tragic outcomes in heart disease in general media and a rising paranoia, we now find ourselves in the midst of an echocardiographic epidemic, fueled by cardiologists, who are unwilling to say “no” to obstetricians who are terrified of missing something. Lastly, we have a system that forgets that over-testing could penalize patients in a variety of ways.
Doctors anxiety masquerading as Protocol
A spade is a spade whether you like it or not. The average Indian obstetrician today is not ordering an echocardiogram because she believes the woman has cardiac disease. She’s doing it because if anything anything goes wrong, she doesn’t want to be blamed for not “having ruled out everything.” In other words, to protect themselves, not the patients. This is classic defensive medicine, induced by aggressive audits of maternal deaths. What was meant to improve care has blunted our common sense. Government monitoring maternal deaths, though well-intentioned, has induced a culture of cover up obstetrics. When outcomes are uncertain and punitive audits loom large, “Do an echo” becomes the safest default.
But this anxiety-driven medicine is not safe. It’s perfect example of ignorance wrapped in a bag of fear. It is sad to note that even experienced obstetricians refer apparently normal pregnant women for routine echo. More curiously some of them are meant to rule out peripartum cardiomyopathy at 24-30 weeks. It sidelines clinical judgment and turns antenatal care into a tick-box ritual. It transforms even highly skilled obstetricians into a panic referral mode. And all the while, cardiologists, many of whom have seemingly disconnected to stethoscopes, happily oblige. (I used to tease my classmate colleague obstetrician, if you really want to rule out PPCM, you need to do serial echoes at least two, one in term and the next after delivery.)
The Cost of Routine
An echocardiogram costs roughly ₹2000 (or even more) in India today. Multiply that by 2.6 crore annual deliveries in India, and you arrive at a staggering ₹5200 crore annually, potentially spent on an investigation that is not recommended as routine by any global guideline, including those from the American College of Obstetricians and Gynecologists (ACOG), the Royal College of Obstetricians and Gynaecologists (RCOG), or WHO.
However, in India, where we are still battling basic issues like iron deficiency, safe delivery practices, and institutional access to labor rooms, many of the obstetricians are casually considering routine echocardiograms as a screening test in pregnant women. That’s not progressive medicine. (*It must be made clear, there are no official guideline that prescribes routine echo in India, but the obstetrician level trend is worrying.)
Let us not underestimate the psychological cost. A vague or equivocal echo report (mild chamber dilation, trace pericardial effusion, mild gradients creates unnecessary anxiety, referrals, and sometimes even unwarranted interventions. These aren’t just academic problems .They can unleash a cascade of referrals, expensive cardiology consults, prolonged hospitalizations fear-induced C-sections, all in women who never need it. Not to forget the worst of all side effects , the fear. A woman who walked into the antenatal clinic smiling, now spends her nights Googling mitral valve prolapse.
We forget that every test carries the burden of interpretation. And in the absence of clinical suspicion, these echoes do more harm than good. They confuse, they mislead, and they medicalize a natural physiological process.
The Misplaced Narrative: Is Cardiovascular Disease the New Villain?
There is a disproportionate narrative emerging in the corridors of public health, that cardiovascular causes are now the leading cause of maternal mortality. Though this is not entirely false, cardiac causes are rising in urban, high-risk populations. But this narrative, when extrapolated to the entire pan Indian obstetric population, is misleading. Most of these studies are from tertiary referral centers, which jack up the true incidence of heart disease in the general pregant population.
Let’s not forget, biggest killers of pregnant Indian women remain postpartum hemorrhage, sepsis, anemia, and eclampsia. These are not fancy diseases. They are diseases of neglect, of systemic failure, of poor infrastructure. Trying to divert funds, resources, manpower, and policy focus from these core issues toward a speculative cardiac screening agenda is not just unscientific, can be unethical too.
Probing the probe
This total dependence on Echo probe, by cardiologists also exposes a deeper malaise. It is the loss of confidence in clinical medicine. Ask yourself, when was the last time a cardiologist palpated a pregnant woman’s apex beat or auscultated thoroughly before performing an echo?
Echocardiography is indeed a quick, non-invasive, accurate tool . We think, there’s little downside for doing it. But this culture is eroding clinical skills. It raises the fundamental question. Have cardiologists lost the confidence to diagnose (or rule out) even simple heart disease without an echocardiogram? This loss of clinical finesse is not just tragic , it is dangerous. It inflates the false positive rate, undermines interdisciplinary trust, and sends the message that technology trumps clinical judgment. It doesn’t.
A Call for Sanity in Science
It is time, we stepped back and asked: what exactly are we doing? Why are we medicalizing normal pregnancy in the name of caution? Why are we spending precious public funds on routine Echo Imaging, when rural PHCs still lack blood banks and partography. Health policy in a country like India must be built on the twin pillars of evidence and equity. Routine Echo fails in both. It is not recommended by global societies, and it redirects attention from more pressing priorities. The answer to maternal mortality does not lie in a Doppler probe. It lies in blood transfusion protocols, nutrition programs, skilled birth attendants, and systemic accountability.
What if if we miss a condition ?
Most young Indian women undergoing childbirth are remarkably resilient physiologically. Even if a minor cardiac anomaly is missed on clinical examination, it rarely alters the course of a normal pregnancy. Ironically, even when we cardiologists do detect such conditions, say, a small ASD or a benign valve lesion we usually end up doing nothing more than “observe” throughout the pregnancy. So the real question is: why are we spending time, money, and emotional burden to look for what we’re not going to treat anyway? Of course, echo is a must in all tertiary hospitals, where high-risk pregnancies are treated.
A request to all Stakeholders
To the Ministry of Health: Please do not be carried away by the seduction of technology. Focus on the basics. Improve the undergraduate education, with a complete overhaul of the curriculum and arrest the shaky clinical foundation. Build safe spaces for childbirth, increase paramedical workers, and establish a speedy referral system. Don’t fall for universal screening of pregnant women with costly gadgets.
To the Federation of Obstetricians: Have courage. Do not let fear dictate your protocols. Stand for rational care, and reclaim your clinical space. Refer pregnant women for a cardiologist opinion, only if you strongly suspect heart disease.
To our esteemed cardiologists: First, spend sufficient time listening to the pregant women , and then therr heart through the Laennec’s device. Record an ECG. 9.5/10 times you can rule out any significant heart disease. If you decide to do an Echo, ensure it’s truly beyond your clinical sense. I know, the reality is much more troubling. Often times, In India, pregnant women are referred to our office only for Echo, they are least bothered about your opinion. (Why I am saying this, because I had a nasty experience with an Anesthetist-Obstetrician combo, who sort of violently argued with me when i said echo is not required in one particular patient. Their concern was, how on earth, I could certify a pregnant women’s heart as normal without doing an Echo.)
To the public : Remember that not everything that can be tested needs to be tested. Sometimes, the best care is less care but delivered with wisdom.
Final message
Indian pregnant women needs true care out of passion, not out of fear. (Which can lead to cascade of inappropriate investigations) Let us go back to the basics and bring down the MMR with mindful allotment of resources, cost rationalization, and technology worthiness assessment.
Further reading
Regitz-Zagrosek V, et al. (2018). ESC Guidelines for the management of cardiovascular diseases during pregnancy. Recommends targeted cardiac evaluation only for high-risk cases. [Eur Heart J. 2018;39(34):3165–3241.]
Siu SC, et al. (2001). Risk of cardiac complications in pregnant women with heart disease. Supports risk stratification, not blanket screening. [N Engl J Med. 2001; 345: 1606–1611.]
Kovács AH, et al. (2014). Guidelines for the management of pregnancy in women with cardiac disease. No support for routine echo in low-risk women. [Can J Cardiol. 2014;30(10):1003–1030.]
Chandraratna PA, Moharir M. (1995). Value of echocardiography in the diagnosis of heart disease in pregnancy. Concludes it is most helpful when clinical suspicion is high. [Am Heart J. 1995;129(6):1115–1117.]
American College of Obstetricians and Gynecologists (ACOG). Practice Bulletin No. 212. Recommends echo only when clinically indicated. [Obstet Gynecol. 2019;133:e320–e356.]
Post amble * Please note : None of the guidelines recommend echocardiography as a routine tool in low-risk pregnancies. All support clinical risk assessment first.
Stent scaffolds are supposed to match the natural size of the coronary artery. Cardiologists take a lot of effort to match stent size and vessel wall. Choosing the optimal size, both width and length, is the foundational parameter. However, there is no perfect match possible with the extent of the lesion.
While stent length mismatch is much more common and taken less seriously,diameter mismatch can be more problematic since it looks strikingly odd & ugly .Still, one section of cardiologists believes a little amount of oversizing is safe and good. There is equal opposition to this concept as well. It is not surprising , acquiredstent-ectasia of coronary artery during PCI ,has both advantages as well as troubling issues.
Please note the (?intentional) proximal LAD pythonisation , by oversizing the stent , which provides more lumen reserve area. What are cost and benefits of this bad principles in PCI practice ? Read below
Advantages of Stent Oversizing
Better Apposition and Expansion
Oversizing can ensure full contact between the stent struts and vessel wall, especially in moderately calcified lesions, reducing malapposition. Prevents stent under-expansion, which is a known predictor of restenosis and thrombosis.
Improved Flow Dynamics
Slight oversizing may restore vessel diameter more completely, improving luminal flow and reducing turbulence.
Reduced Risk of Stent Edge Dissection(in selected cases)
If stent is properly deployed and well apposed, oversizing slightly may prevent gaps at the edges where dissection can initiate.
Helpful in Plaque Compression
Facilitates better plaque redistribution and compression, especially in fibro-calcific lesions.
Disadvantages of Oversizing
Risk of Vessel Injury or Perforation : A stent that is too large can overstretch the vessel, causing deep medial injury, dissection, or even perforation especially in fragile vessels or older patients.
Increased Elastic Recoil : Oversized stents in small or elastic vessels (e.g., RCA) may provoke recoil, paradoxically reducing the luminal gain.
Edge Dissections and Geographic Miss : If oversizing leads to excessive radial force at edges, it can cause edge dissections, especially if not well matched with tapering vessel anatomy.
Neoatherosclerosis and Late Malapposition : Chronic vessel injury from over-expansion may lead to inflammatory changes and promote neo-atherosclerosis, stent fracture, or late acquired malapposition.
Stent Fracture Risk : Over-expansion of certain stent platforms beyond their elastic range increases risk of metal fatigue and fracture, especially in tortuous or mobile segments.
Final message
De novo coronary ectasia is quite a common and fairly benign entity seen in 20 to 30% of normal coronary arteries. However, acquired ectasia (stent-ectasia) can’t be taken lightly. No one can predict who is going to accrue the potential benefit and risk. Slight oversizing of stents (typically within 0.5 mm above reference vessel diameter) can be beneficial in selected clinical situations, such as in fibrotic or calcific lesions, or in large proximal segments. However, it must be done cautiously, guided by imaging (IVUS or OCT), and never exceed the manufacturer’s recommended expansion limits.
This IVUS-based study on nearly 3,000 lesions found that slight stent oversizing (within 0.5 mm of reference diameter) led to better stent expansion and lower restenosis, without increasing complications.
This landmark randomized trial (IVUS-XPL) showed that IVUS-guided stent sizing often resulting in slightly larger stent selection and greater expansion reduced major adverse cardiac events significantly at 1 and 3 years.
Post-amble
Can we do an intentional post-dilatation to increase the lumen size in small vessels ?
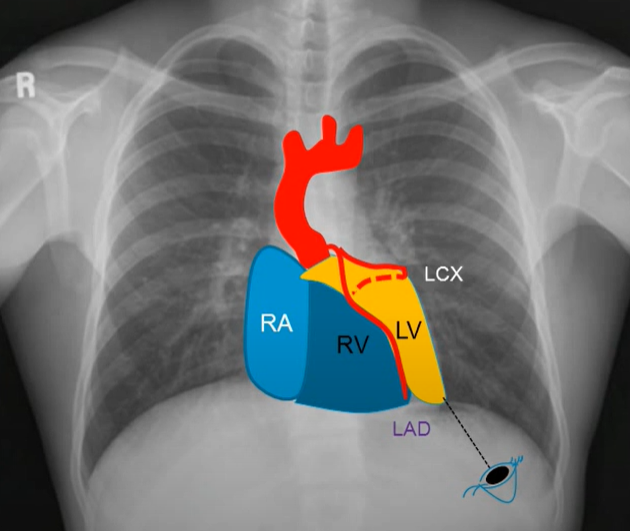
Though we do coronary angiogram and complex angioplasties day in day out, we rarely get oriented , to the exact anatomical relations of individual coronary artery with reference to cardiac chambers. When I asked my fellows, to identify , the chambers on either side of left main at its bifurcation , none of them were confident. (I must confess, I was also in the same page of vagueness till I saw this clip .)
A brief anatomy of LCA
*LMCA after emerging from the aortic sinus, the travels a short distance, usually between 5 to 15 mm, towards the left side of the heart. During this initial course, the LMCA passes posterior to the pulmonary trunk. The left main is also closely related to RVOT especially the posterior and septal aspect. Once bifurcated , the LCX is related to LAA.
LAO caudal view : The most familiar, and usually the first shot we do.
This video clip is posted here with the courtesy of Dr. Srinivasa Prasad, from Sri Chitra Thirunal Institute of Cardiac Science, Thiruvananthapuram, India from his you tube post.
Note : In LAO caudal view, we are looking from the left side, from below near the spleen, towards the right shoulder. The anterior structures will come on the left side and all posterior strictures fall on the right side of the image.
The yellow Zoneis a wide area between LAD and LCX that engulfs the whole left ventricle. The blue zone is the anteriorly placed RV, especially the RVOT, which comes closer to the left main. The one below the LCX is the posteriorly placed left atrium depicted in green zone. (Not in above picture)
Clinical Implication
As cardiologists, we literally camp inside the coronary arteries with various weaponry and ammunition. It is always wiser to know the surrounding structures, as the risk of Injury hangs like a Damocles sword . Intra-cavity perforation, though rare, can still occur, and many are not recognized because they are well tolerated. Structural interventions like LAA closure and RVOT ablations can directly pose a threat to the left main or LCX, respectively.
Final message
Getting oriented to three-dimensional coronary arterial anatomy, is indeed a tough task. Those who are able to do it, add critical value to their interventional prowess. It is good , if we try identify cardiac chambers in each coronary angiogram shots.
The National Eligibility-cum-Entrance Test (NEET-UG) was introduced with the promise of ushering in fairness, standardization, and meritocracy in medical education across India. At first glance, it appears to have succeeded — replacing state-level chaos with a national-level uniform entrance system. However, a deeper analysis reveals that NEET has also created a more insidious structure of exclusion and privilege, particularly through its poorly understood and easily manipulated 50th percentile eligibility criterion. This mechanism has inadvertently (or perhaps intentionally) legalized the backdoor entry of underqualified but wealthy candidates into private medical colleges, all while marginalizing thousands of meritorious but economically disadvantaged students. What we are witnessing is not an accident of policy but a systemic betrayal of the very values NEET claims to uphold.
The core issue lies in the use of the 50th percentile as the qualifying benchmark, rather than a fixed percentage of marks. In a pool of over 12 lakh test-takers, this means nearly 6 lakh students qualify each year, while India has only about 1 lakh MBBS seats — half of which are in government colleges. This creates a vast pool of surplus eligible candidates.
One may argue that such a buffer ensures inclusivity and provides opportunities for students to enter allied medical fields. But in reality, this bloated qualification base primarily serves a far more cynical purpose to feed the commercial engine of private and deemed universities. These institutions, often owned by political syndicates or business conglomerates, need legally “eligible” students to fill their overpriced seats. Thus, NEET’s percentile-based qualification becomes the legal stamp that converts a failing candidate into a paying customer.
The biggest beneficiaries of this system are clearly the private medical colleges. TheY exploit the legitimacy provided by NEET qualification to offer seats to candidates with ranks as low as 5.5 lakhs This is not an aberration; this is the business model. The eligibility net has been cast so wide that even students performing in the bottom 10% are now a valuable market segment for these institutions.
Politicians too have their share in this ecosystem. Many private medical colleges are directly or indirectly operated by political trusts. These institutions flourish under regulatory blind spots and benefit from policies that expand eligibility but do little to control quality. The illusion of merit-based admission helps them deflect criticism while quietly preserving a robust revenue stream. Middlemen, agents, and education consultants also thrive in this system, legally brokering “management quota” admissions for candidates who would otherwise never see the inside of a medical college based on academic merit alone.
The tragedy is not just in who gets in, but in who is left out. Consider the student ranked 45000, who misses a government seat by a few ranks and cannot afford the exorbitant private fees. Meanwhile, a far less qualified peer with is ranked beyond 5 lakhs buys entry into the same profession. The idea that NEET ensures equal opportunity collapses in the face of such economic discrimination.
This skewed dynamic does not merely harm students .It damages the very fabric of the medical profession. The country is gradually producing doctors who may not have entered the system based on ability or passion, but because they could afford to. This threatens the ethical, academic, and clinical integrity of the profession. Over time, it will erode public trust in doctors and healthcare itself. Furthermore, the use of wealth to bypass academic rigor is fundamentally anti-Constitutional. Reservation in education is meant to uplift the socially backward, not to empower the economically elite. By allowing rich mediocrity to flourish, the NEET system insults both merit and social justice.
The system’s design is cunning in its illusion of fairness. NEET’s structure with percentile-based eligibility, decentralized counseling, and layered quotas appears technical and neutral. But it’s a carefully crafted mirage. The Supreme Court rulings that upheld NEET (TMA Pai Foundation vs. State of Karnataka, 2002; and Christian Medical College vs. Union of India, 2020) emphasized fairness and uniformity. Yet today, the same system legally validates an admission model where the top 10% merit students compete for government seats, and the bottom 40% enter through payment, wrapped in a veneer of legitimacy.
NEET should be made as entrance test not eligiblity test
It is time to end this farce. The first reform must be simple but fundamental: eligibility should match seat capacity as UPSC,IAS exams. Only students up to 1.2 times the total number of MBBS seats should be deemed qualified. This ensures that only competent and competitive candidates enter the counseling process.
If India truly wants to select its doctors based on their wisdom and dedication, and not the power of the bank accounts, it must rethink NEET’s qualification model. Otherwise, the country is heading toward a future where healthcare is not just privatized but intellectually bankrupt.
Final message
NEET as model for national entrance is welcome But, only the methodology is wrong .
Realise , when some one says they cracked NEET, by merit, it may sound as if they conquered mount Everest.
Do you know , what exactly it meant this year? All that is required, is to score atleast 144 out of 720 , ie 19% marks, a score, even the back bencher will be ashamed to tell.
It is strange , only medical profession suffers from this.Can you ever think of buying an IIT, Charted accountant or IAS seats , by making lakhs of students eligible through percentile system of examination ?
References
National Medical Commission (NMC) Regulations on Graduate Medical Education (2023).
Supreme Court of India. Christian Medical College vs. Union of India, 2020.
Medical Council of India data on MBBS seats: www.nmc.org.in
Times of India (2023): “70% of private medical college seats filled by students with ranks >4 lakh”.
Current generation doctors are gifted, can be immensely proud to practice medicine with cutting-edge technologies and advanced medical therapies .Today is the official doctors day in India, in honoring one of most great physician of our times Dr.B.C.Roy on his birth day.
Who celebrates Doctors’ day and for what ?
Sharing here , one of the deeply reflective article about, reality of being a doctor today. Published in today’s Hindu, (July1 2025)India’s National New paper, Opinion Column by Dr C. Aarvinda . It is a 6 minute read, must for all those who truly love our profession.
Courtesy : Dr.C.Aravinda MD, Assistant Professor of community medicine. Thanjavur medical college. Tamil Nadu .India.
While the profession is glorified at every level, there seems to be little to celebrate at a personal level. The same public who celebrate doctor’s day , become a mute witnesses to innumerable attacks unleashed on them on a day-to-day basis across the country. It is a sad truth the medical profession has been hijacked, far away from its original intended destination by both visible and Invisible forces. Many honest, hardworking, and humble doctors are compelled to traverse a turbulent moral landscape.
Final message
Doctors’ day celebration is meant for whom? Realistically, it is the occasion for patients who respect and show love to their healers. The whole idea got distorted in recent times. Definitely, it is not meant for pride hunting and forcible Intrusion by the industry , into the noble profession.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.










{kind=link}