Pulmonary embolism continues to be an intriguing entity, both in the diagnosis and management. The spectrum is wide, from a clinically insignificant, or totally unrecognized episode to a massive cardiopulmonary event causing sudden death. Similarly, treatment can either be conservative (even sending the patient home ) or lead to aggressive cath lab intervention.
The task of PE risk stratification
Obviously, risk stratifying is the mainstay in the management.The fact that we are grappling with multiple risk stratifying scores like PESI, simplified PESI or HESTIA expose our limitations. To segregate , low and high‑risk categories do not demand much expertise. It is the intermediate‑risk group that plays havoc in the ER. It is based on RV function and biomarkers like troponin and D‑dimer. But it was soon realised clinical parameters like blood pressure and hemodynamic stability are the more powerful markers of risk.
However,the reality is, many patients in the intermediate‑risk group are rushed to the cath lab, either due to overestimation of risk or fear of potential escalation to high risk. A third reason,is often non‑academic, it’s done for showing our expertise.
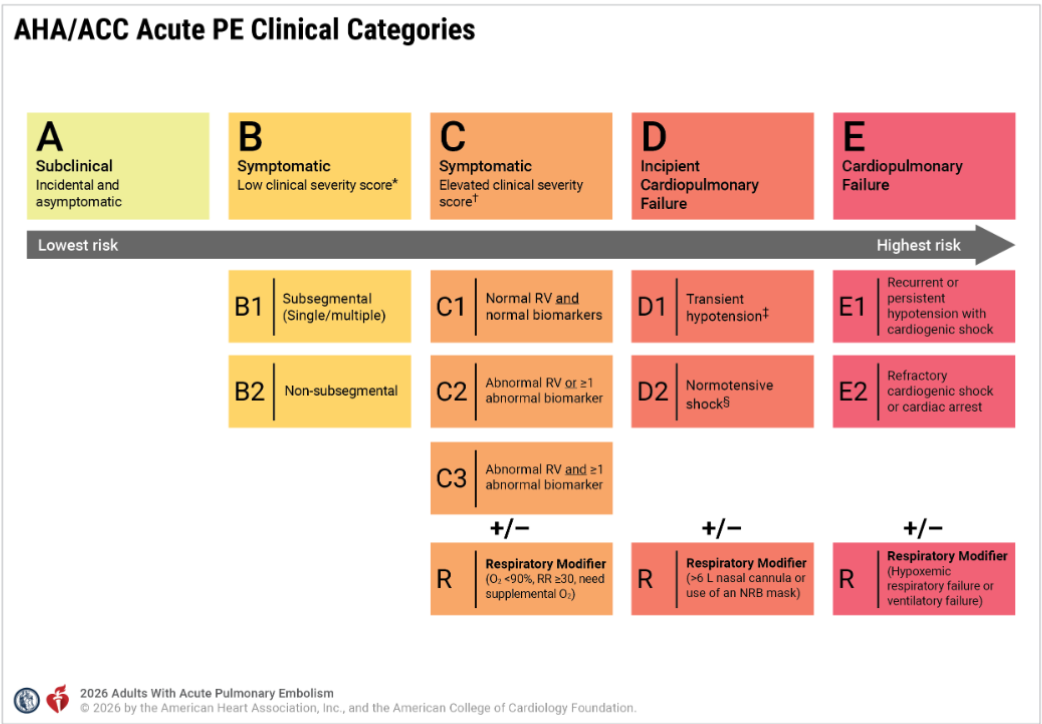
Now, to solve the puzzle of intermediate risk, we have created two new subcategories, C and D. ACC/AHA has been very careful in defining and labeling the entities. Still, there are a lot of gaps that need to be fixed.
In this post let us confabulate few aspects of the new grading of PE and in particular the curious case of D 2 shock .
series of iFAQ ( infrequently) asked questions will from the basis of this discussion
Does category C to D progress in a sequentially worsening hierarchy?
Though it looks that way, the clinical presentation rarely follows a sequential order.
Why is BP is not given adequate weightage in Category C?
A normal blood pressure is a mandatory baseline requirement to enter Category C. However, BP is an important factor used in the clinical severity assessment (PESI etc) .It is not clear why , the committee did not explicitly use the term Category C with reference to BP.
Why is the word “symptomatic” missing in Category D?
The word “symptomatic” is deliberately omitted from the title and subcategories of Category D in the 2026 AHA/ACC Pulmonary Embolism guidelines because symptoms alone are no longer a differentiating factor at these higher levels of severity. Alos, the patient needs to be alert, to tell the symptoms.
Does that mean symptomatic Class C is less risky than asymptomatic Class D?
Yes. A symptomatic patient in Category C is at a significantly lower risk of dying or collapsing than a patient in Category D.A patient in Category C might feel worse because they are aware of their chest pain. A patient in Category D may not complain of pain at all, perhaps because they are in altered sensorium.
What is D2 shock, and when and how do we diagnose it?
First, the patient must fulfill the baseline criteria of Category C, which includes right ventricular dysfunction and positive biochemical parameters of either Troponin or NT-Pro BNP. Then, they must have at least one parameter to confirm shock. Under Category D, the term normotensive shock defines the D2 category, where the blood pressure is normal.
The signs of shock include:
- Lactate greater than 2 mmol/L.
- Evidence of acute kidney injury, meaning urine output is less than 0.5 mL/kg/hr.
- Altered mental status changes.
- A cardiac index less than 2.2 L/min/m2.
- A mean arterial pressure less than 60 mmHg.(In D2 shock the MAP more than 60 mmhg)
Is elevated lactate mandatory to diagnose D2?
No. Any single criteria from the above list is enough. Oliguria alone or even altered mental status is sufficient.
Can D2 shock be diagnosed based only on altered sensorium?
Yes. it is possible to diagnose Category D2 based only on a vague, mild, or temporary change in mental status .This carries a huge risk of falsely classifying a stable Category C patient into the more critical Category D. To prevent this error, the 2026 AHA/ACC guidelines has strict definition of Category D2, ie the altered sensorium must be profound and persistent.
Why Category D1 patients can show a fall in BP, while Category D2 has normal BP?
In PE, the right heart is overwhelmed by the acute rise in RV afterload, causing a short term drop in the volume of blood until the RV recovers. This is the mechanism of fall in BP D1.In Category D2, the blood pressure stays completely normal (90 mmHg or higher), but the patient may be in ongoing organ shock spiral. In D2 the RV is failing just like in D1, but the patient’s sympathetic response fires at it’s peak with maximum vasoconstriction to sustain the BP and life.
Why D2 shock sounds a mystery ?
It may look implausible that a patient in D1 can have low blood pressure, but when they worsen, they seemingly gain blood pressure to reach D2 and get the tag of normotensive shock. In the bed side this is not true. The hidden clinical reality is, D1 and D2 are not meant to be viewed as sequential, worsening hierarchical stages. A patient can move from Category C to D1 or D2 directly, and a direct jump from Category C to Category E is also possible without spending any time in Category D.
Dynamics of the C-D-E categories
It becomes problematic to have the term normotension in the title itself in D2 . This implies ,a patient with hypotension and underperfusion should exit from D2 shock. This could mean a worsening patient paradoxically enters Category D1 or Category C or E. To be precise, a fall in blood pressure represents is really a sign of worsening or not is debatable and decided on patient to patient basis. Also both category C will also feature a normal blood pressure. This can be mixed up with D2 if organ perfusion markers like oliguria occur transiently. This trichotomy between hemodynamic stability, organ perfusion , versus respiratory stability needs to be addressed. The PERT team need to be vigilant on this asseement.
Do we need to sub classify D2 shock ?
In realistic observations, the most common cause of normal BP in D2 shock is the intensive treatment these patients receive with RV inotropes and systemic catecholamines. Perhaps we may need to add another rider to Category D2, such as Normotensive with drug support versus normotensive without inotrope support. This would help us know the exact direction in which these patients will progress.
Can Category C3 be riskier than D2?
This is tricky and indeed seems possible . Category C3 can exceed the morbidity of Category D, especially when it features the respiratory modifier as C3R. It must be recalled that both the C and D categories present with right ventricular dysfunction and positive cardiac biomarkers, but their primary organ failure differs. A Category C3R patient experiences an acute oxygenation crisis. Conversely, a Category D2 patient, even with normal lactate, suffers from occult circulatory shock (an adequately functioning liver can clear the lactate efficiently.) Though C3R appears more dramatic at the bedside due to the need of respiratory support , Category D2 carries a higher mortality.
Final message
“It looks like treating patients with PE is much easier task than risk stratifying them“
Pulmonary embolism management is a fierce fight between the right ventricle, the occluded pulmonary arteries and the lungs.The first 48 hrs is crucial. RV shock incidence rapidly reduce after this time window. We realised very late, the total thrombus burden actually has a poor correlation with the final outcome. Most episodes of PE can be managed medically.
Balancing pharmacological lysis versus catheter-based lysis requires a very delicate skill. While most patients are eligible for standard lysis, only a very few truly benefit from catheter-based therapies. The rate of RV failure and mortality drops dramatically once the right ventricle rises to the challenge. Therefore, there is no clinical point in doing a catheter-based lysis if the blood pressure is normal and the right ventricle is already recovering.
Finally and most importantly, the alarming entity D 2 (Normotensive shock) should not cause unnecessary panic. If the, saturation and RV function remains good or shows signs of recovery , catheter based modalities can be avoided.
Reference
3.Dominick Roto, Raquel Lamarche, Navigating normotensive shock Chest physician May 6, 2026



