We learn from basic physiology lessons that human body is made up of 60 % water. What about heart ? There is no reason for the heart should behave differently from rest of the body . If my assumptions are correct when the normal heart weighs 300g , 180g of which should be be water. The same thing could be applicable for LV mass( * Reference requested)
Is there myocardial congestion in cardiac failure ?
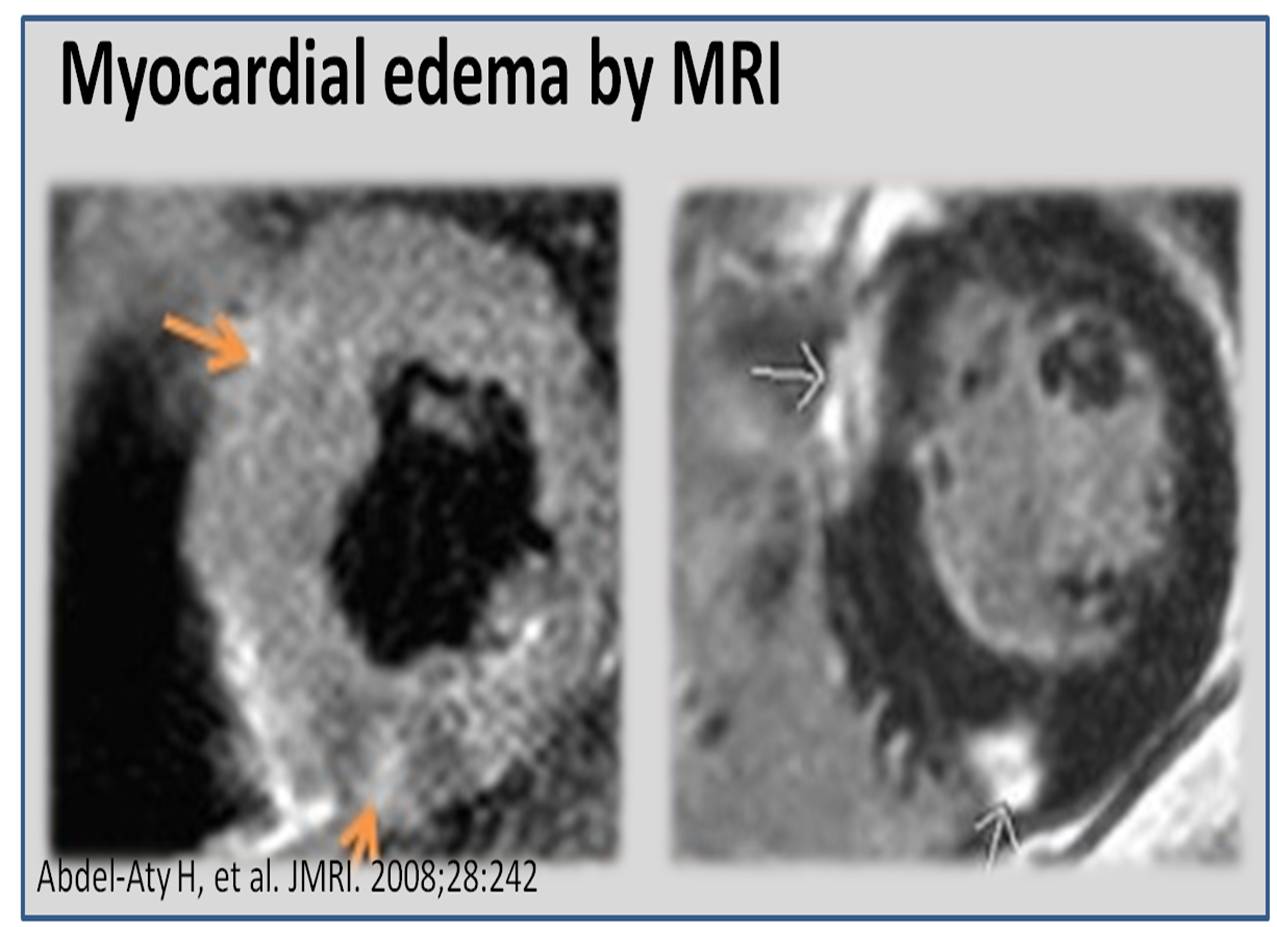
Genesis of edema in any tissue depends on local hydrostatic pressures, tissue resistive forces, osmotic balance, and cell membrane permeability. In the myocardium individual contribution of above factors are not known. Apart from total myocardial water content , myocardial water logging depends upon the trans myocardial venous gradient and the coronary sinus exit pressure in right atrium.Technically ,any severe right heart failure should lead to myocardial congestion at least to some degree.Unlike the lungs , the myocardial edema fluid doesn’t produce crackle , (May cause S -3 gallop instead) . However ,we have modern technology to image water inside the myocardium. Yes, it is called proton / hydrogen imaging or simply called MRI .
This is especially evident In chronic kidney disease , where in the fractional water content within the myocardium is expected to increase further as the whole body is water logged.
We have seen time and again patients with CKD improve in LV function immediately after dialysis . It happens like a magic . The mechanism is simple .The over-hydrated cardiac Interstitium threatening to drown the myocytes is promptly dehydrated by dialysis. This was my wild guess until I came across this paper which proved the exact points.

Other situations where myocardial edema may play a significant clinical Impact (*Includes increased permeability of myocardial capillaries)
- Myocarditis
- Transplant rejection
- Stress cardiomyopathy (Takotsubo)
- Congestive heart failure
- Acute ischemic injury
- No Reflow situation after PCI
Final message
Myocardial interstitial edema in cardiac failure is a grossly under diagnosed entity. A water-logged myocardium is classical at least in CKD. We know it can severely compromise the LV function especially, the diastolic function that explains the all too common flash pulmonary edema in CKD.
The number of studies in this topic (Myocardial Hydrology !) is minuscule compared to other areas of research in cardiology literature.There is a need to involve both Nephrologist and cardiologists to explore this curious concept of dialysable left ventricular mass in CKD/Cardio renal syndromes !

One more area of research
It is reasonable to believe, cardiomegaly in cardiac failure is primarily related to the increased end diastolic volumes .Still , we are not clear whether there is net increase in cardiac mass as the surface area of the heart increases with dilatation. (Even in DCM ? ) Whenever myocardial mass increases relative increase water is likely. Does the beneficial effect of diuretics in cardiac failure , and the restoration of LV dimension is due to myocardial interstitial diuresis as well ?
Reference