One of my favorite quote about Happiness from Buddha !
Posted in Uncategorized, tagged happiness quote, happy doctor on September 25, 2014|
Posted in Uncategorized, tagged Mechanis m of tall T in hyperacute MI stemi on September 10, 2014| 1 Comment »
Most of my students were struggling to answer this seemingly simple question . I realised later it is indeed a difficult one !

Some thoughts
Tall T waves are observed in very early phase of STEMI .(Within 30 minutes ?) What is the mechanism ? Since ST shifts occur little later than T elevation ( considerable overlap may occur) it may not be related to current of Injury.It is an inherent alteration in the T wave genesis .T wave is inscribed when rapid phase 3 K+ efflux happen (Mainly by Iks and also IKr )
What is the effect of ischemia on K + channels ?
No uniform answer.(Blocks, stimulates, irritates, Bi-phasic, variable ?)
There are 6 important K channels in every cardiac myocyte adding to the complexity.
Does the Ischemic cells leaks potassium or accumulates it ?
Though It does both , predominantly it should leak .If it’s leaking there is local extracellular hyperkalemia . Is that the explanation for tall T waves ?
What is the influence of QT interval on T wave morphology ?
Long QT as occurs in hypokalemia pulls the T down and it may even invert it. .Short QT tends to push it up as in ERS .The effect of ischemia on QT interval is again unpredictable.Further regional and remote ischemia in a given patient can alter this.
Once the ST begins to elevate the T waves losses it power to grow tall .It only can regress. I think this is the time the QT is sort of prolongs .
Effect of reperfusion on T waves
The tall T tend to regress as some form perfusion takes place as K+ Is pushed back into the cells or flushed away from the vicinity.
The dynamic nature of reperfusion makes the behavior of T wave amplitude further complex. But one thing is certain , a well perfused IRA is associated with inverted T wave which we call it as completion of the process of evolution of MI .
Finally and most importantly this hyper acute T phase is not a constant phenomenon. In fact it is uncommon in persons who have baseline T inversion .After analysing many things we are back to the original state of ignorance .
Summary
Researchers with intra-myocardial micro electrodes try to decode the mysteries in electrophysiology . Still there is a huge disconnect between clinicians and physiologists.
In simple terms I would believe the mechanism of ischemic tall T waves are almost similar to renal hyperkalemia. (A local , transient extracellular k + excess ) The base of the T waves are not narrow and tented as in CKD because some degree of ST elevation (that always is expected ) widens the base of T wave. Further ,the prolonged QT interval in renal hyperkalemia stretches the QT and encroach the base of the T wave to the left making it appear narrow.
A simplest version for students
Tall T waves are due to transient local extra cellular hyperkalemia , when K + leaks due to cellular Ischemia.
Caution: This is a superficial scientific attempt .I need inputs from more scientific brains and electrophysiologists.
Read further
Posted in cardiac resynchronisation, Cardiology - Electrophysiology -Pacemaker, tagged crt vs icd, when should i use combo device ?, when should i use crt and icd ? on September 5, 2014| 1 Comment »
CRT is done for advanced heart failure to improve exercise capacity and hence the quality of life .It does not do any thing significant in prolonging life .ICD is again implanted in advanced LV dysfunction with either documented VT/VF or patients who are at propensity for VT .It has dramatic benefit in preventing sudden cardiac death.
Both CRT and ICD has some overlapping indication in cardiac failure. Attention young cardiologists, please realise among these two the value of ICD is many many fold higher than CRT.This fact is rarely discussed and disseminated.
True benefits of CRT is realised only when it is combined with ICD.
Summary
*Except in patient with degenerative complete heart block , both ventricles are paced the term Bi-Vi pacing is used instead of CRT.Since LV function is normal here , there is no de-synchrony in the first place .The synchronised BIVI pacing is meant to prevent future heart failure
Final message
Always use a combo device in advanced symptomatic heart failure which is refractory to medical therapy.
After all , there need to be a life in the first place so that we can improve it . ICD ensures life while CRT tries to improve it.
Posted in Uncategorized on August 31, 2014| Leave a Comment »
The correct answer could be any of the above , depending upon the level of your knowledge.
Ever since Herrick reported coronary thrombosis as a cause for MI and Davies documented it by angiogram many decades later (1980) ,the fate of thrombus and the mechanism of its dissolution is the key to our understanding of ACS.
Even though we are now able to take on this thrombus in a direct fight by aspiration techniques ,still the hematological aftermath and the aberrant coronary behavior can fool us at any time ! The major lesson learnt in recent times is the success of pPCI is not in clearing the thrombus but ensure it never accumulates again at the site in the future .This is why there is whole big industry working on post PCI anti coagulation and anti platelet strategies .
Clinical correlates of poor perfusion in micro circulation.
Plugging of micro circulation is the most under-recognised issue.This results in no reflow in acute fashion or LV dysfunction and micro-vascular angina in long term . Late recovery of LV function is attributed to late clearance of thrombotic debri.
RCA vs LCA thrombus load.
*One interesting observation is RCA thrombus clears more slowly as it has no well formed venous circuits .most RCA blood drains through thebesian veins which traverses RV myocardium .this can be hemodynamic hurdle unlike the LCA venous drainage
Posted in Uncategorized on July 31, 2014| Leave a Comment »
A tense anesthetist calls for help !
I had an unusual cardiac consult last week .A middle aged man who was to undergo routine ortho surgery wanted a cardiac clearance.
It was a through and through fracture of clavicle , why do they need a cardiology opinion , it seemed a simple procedure I asked over phone
The anesthetic fellow who was in charge of the patient told me ,”There is a wire just going parallel to the clavicle sir .I believe it is pacemaker lead” I agreed to see the patient immediately
This was the X-ray
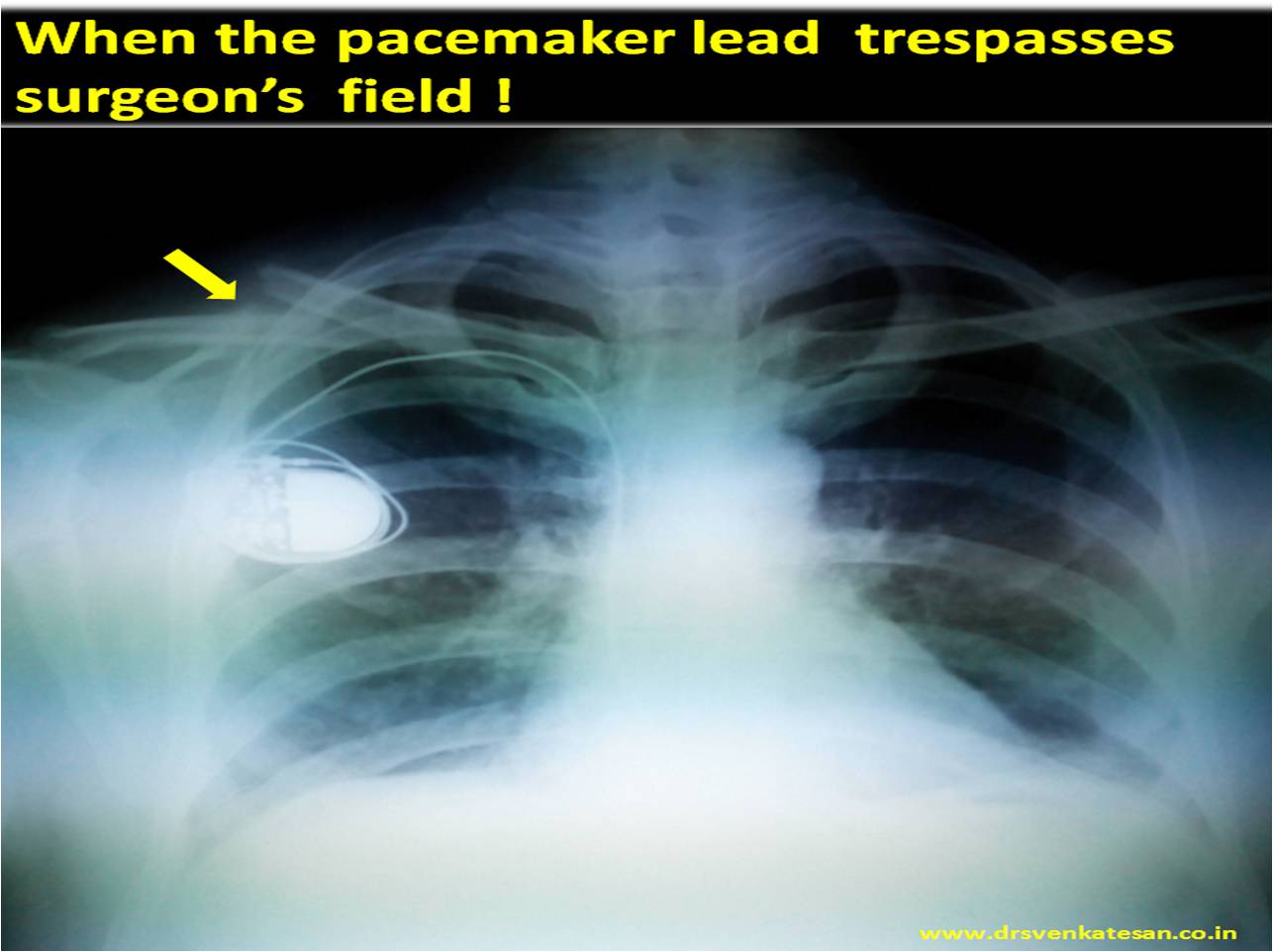
It was obvious why they got tensed up as the pacemaker wire criss -crossed surgical field . His ECG showed own rhythm of 80/minute but occasionally VVI pacemaker was capturing his ventricles.
I suggested
General precautions
Use of magnet in such situations (Link to magnet and Pacemaker)
Keeping a magnet over the pacemaker generator removes the pacemaker sensing function and is an option if prolonged electrical interference.
*Caution : Response to magnet can be quiet variable .Should be done only with cardiologist supervision.
What happened to this patient during surgery ?
Nothing alarming.When anesthesia was induced he was entirely on pacemaker rhythm . limited cautery was used with ease. Patient tolerated well.
Final message.
One need not panic when a pacemaker patient is taken up for non cardiac surgery .It is not a major issue .Few precautions are required .
Read a related article in this site .Electrical cautery in pacemaker patients.
Reference

Posted in Brugada syndrome, Cardiology - Electrophysiology -Pacemaker, tagged brugada syndrome, camel sign in brugada, response to excercise and brugada, risk stratification of brugada, tmt and brugada, what happens to st elevation in brugada after est tmt excercise on May 31, 2014| Leave a Comment »
Brugada syndrome has three distinct type of ECG pattern.ST segment in V1 to V3 shows the maximal changes .All manifest as subtle forms of ST elevation .
This is an ECG of a young male who was suspected to have CAD with an abnormal ECG .(Which was Infact Brugada . )

He was adviced EST by a physician .Compare the leads V1 to V3 pre and post exercise

Prompt normalization indicate correction of repolarization heterogeneity and suggest relative immunity for development of ventricular arrhythmia at fast rates.
In contrary , new appearance or worsening of Brugada pattern would help us identify high risk subsets of Brugada.
Message : We have sophisticated genetic and EP studies available EST is a simple test to risk stratify these individuals.( Not a perfect screening test though !)
Reference
1.Grimster A,Segal O,Behr E. Type I Brugada electrocardiogram pattern during the recovery phase of exercise testing. Europace 2008;10:897–8.
Posted in Uncategorized, tagged Ischemic RBBB, lbbb vs rbbb, rbbb and stemi, right bundle brnch block ischemic on April 11, 2014| Leave a Comment »
A 76 year old man with history of recent stroke presented with acute chest pain and his ECG showed ,
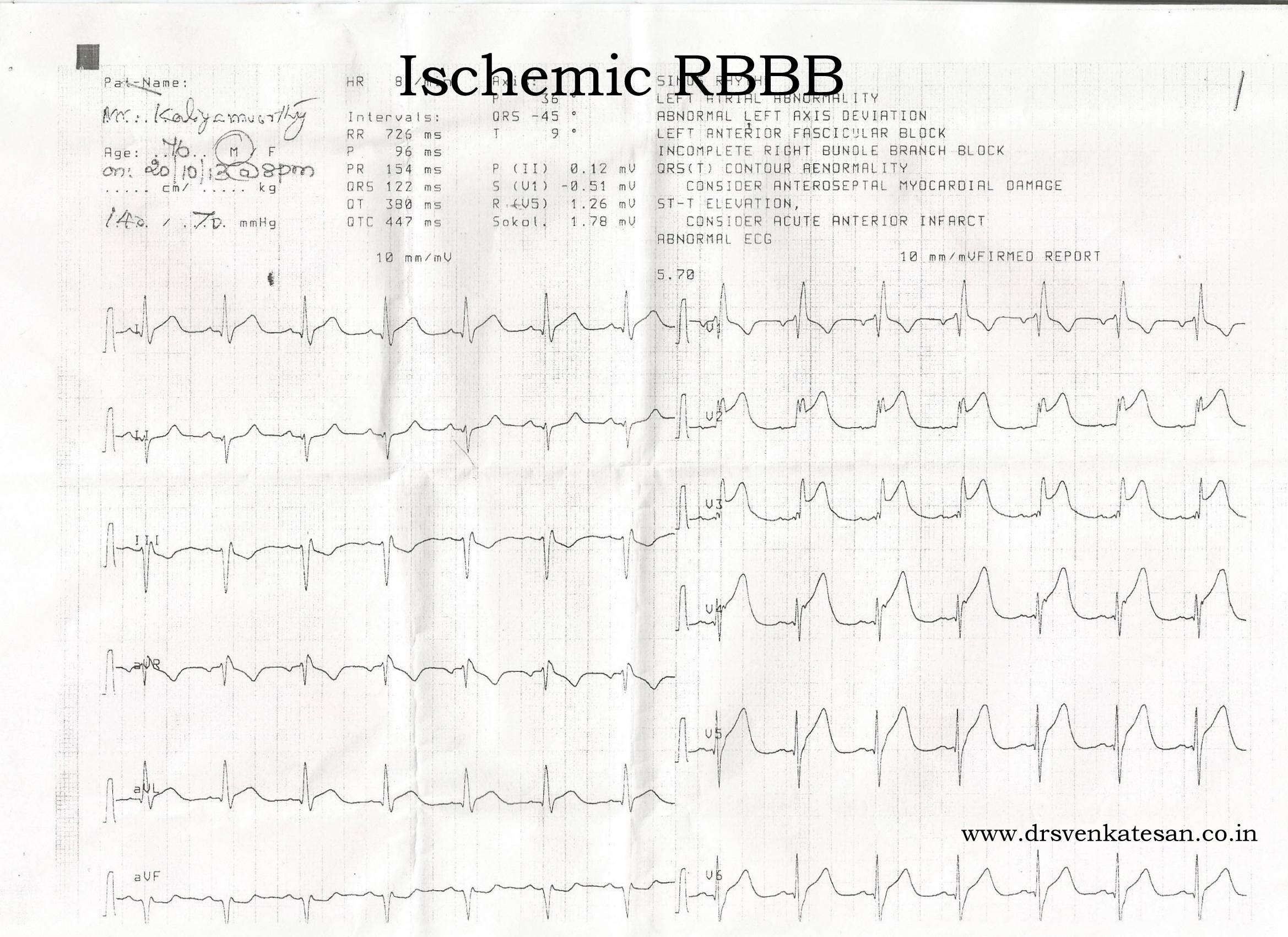
It was diagnosed as Anterior STEMI .Since he had co-exciting renal dysfunction also he was not considered for thrombolysis (Primary PCI not feasible !)
IV Heparin bolus followed by infusion was started. Patient had a comfortable night stay. The ECG taken on the morning looked like this.
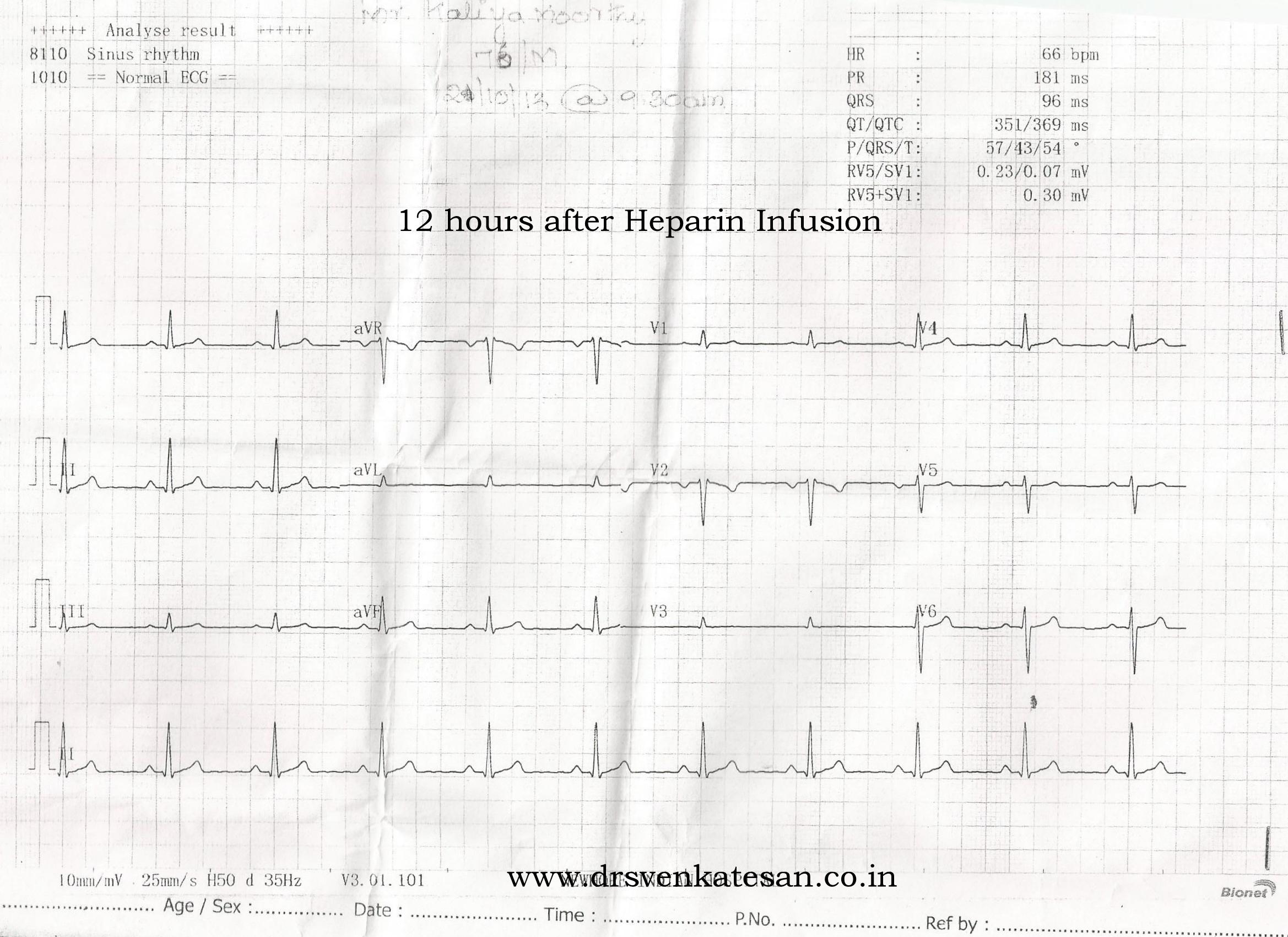
Do you call this aborted STEMI or a simply an Ischemic RBBB ?
Transient RBBB due to Ischemia in LAD territory(with septal compromise ) is very much possible during ACS. But , it is a rarely discussed entity unlike ischemic LBBB .
We know qRBBB complicating anterior STEMI is much commoner than LBBB , still transient ischemic RBBB in non STEMI setting seems to be uncommon .Is it possible propensity for Ischemic RBBB is different from necrotic RBBB ?
Posted in Uncategorized, tagged best cardiac drug, cardiac pharmacology, frusemide, frusemide heparin aspirin, greatest cardiology drug on February 16, 2014| Leave a Comment »
Cardiology as a filed has been the epitome of progress of medical science in the last century .Most research in cardiac science has grown and transformed with a definite clinical purpose.
The cardiac pharmacology has grown many fold and various drugs play a distinct role in relieving symptoms and prolonging life .
Which drug , do you think has the maximum impact in the clinical outcome and overall cardiovascular health of our population ?
My vote is for the old warrior . . . yes the the drug , which is used atleast a million times a month to unload the heart the meanly loop diuretic Frusemide ! Heparin came very close second !
Posted in Cardiology classics, Cardiology-Land mark studies, cath lab tips and tricks, Great Men in cardiology, history of cardiology, Land mark articles in cardiology, Uncategorized, tagged concept of physician assistant, dr stead eugene anson, father of physician assistant, grady memorial hospital atlanta georgia, history of cardiac cathetrisation, right heart catheterisation on February 16, 2014| 1 Comment »
Today , we post cases for coronary angiogram , just like sending clients to breakfast table ! Close your eyes. Think for a moment. It is heartening to know how cardiac catheterization grew from a humble beginning . We know , Forssman , Cournand and Richardson who shared the Nobel price for Inventing cardiac catheterization in 1930s .
Soon after it’s invention it was criticized by most, few ridiculed it outright , few others wondered about it . One man from the iconic Grady memorial hospital , attached to Emory silently adopted this procedure and almost single-handedly did more than 1500 cardiac catheterization procedure. (Between 1940-50s)
How many of us know this man from Atlanta ,Georgia ?
Some times history appears unkind. He is Dr Steads . . . to be precise Dr.Eugene Anson Stead Jr. ( 1908, – 2005)
Born in a humble background in the suburbs of Atlanta , became a great medical teacher , researcher and educator . He is one of the founding fathers of cardiac catheterization . Defined it’s usage in clinical cardiology . The other major achievement was his strong conviction that medical science is indeed simple but made complicated by complex concepts .This thought transformed in him , as he found the concept of physician assistant . He believed focused medical knowledge in young and enthusiastic mind can make huge difference in the way medical knowledge is disseminated, applied and consumed .What a stunning truth even today !

The legacy of Grady continues which is one of the largest public hospital in USA with special affinity to poor and low-income population.
The lab which Dr Stead worked was later taken over by Dr Noble O Fowler* , another great cardiac physician continued the research and wrote the famous book on cardiac diagnosis and treatment.( * I think it should be in early 1950s when Dr Stead left for Dukes)
Final message
Invention of a concept is one thing . Accepting it , trying it , improving it , disseminating it , is an equally important contribution to science. Dr Stead did exactly that .He remained a positive force in propagation of medical knowledge, made it available for those people who need it .
He passed away on June 12, 2005 at the age of 96 leaving behind a huge legacy .It will be an error if we don’t teach our young students history of such great men , in medical schools today !



