“Nothing moves without an external physical force”
SCAD is a popular entity among cardiologists in angiographically sub-categorizing of ACS, especially in women. The entity is indeed important to recognize, as the otherwise omnipresent PCI, is contraindicated in SCAD.
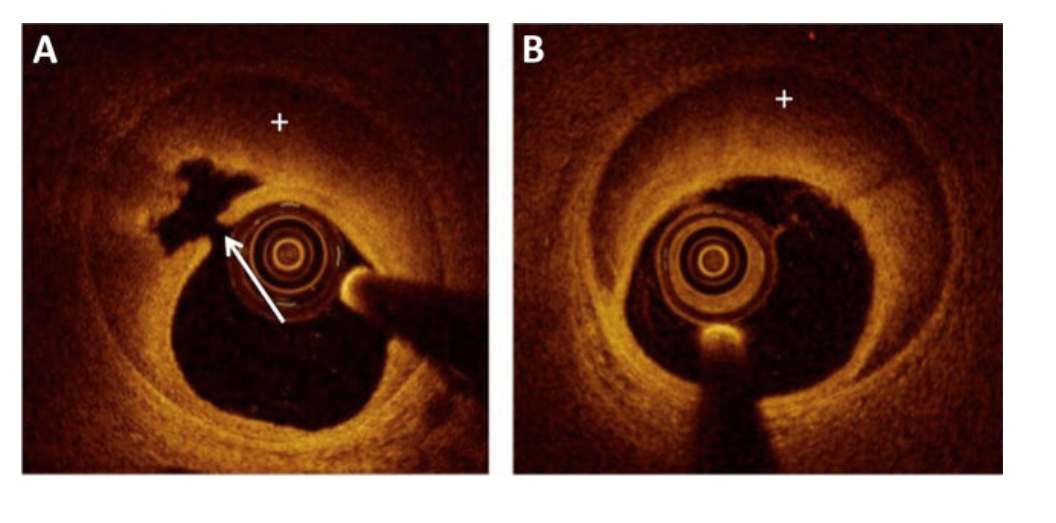
Meanwhile, we can’t take every suspicious-looking dissecting flap as SCAD in women. The word spontaneous in SCAD, could often convey a potentially erroneous meaning, for the simple reason, plaque ruptures and fissures that triggers dissections of varying lengths can be spontaneous as well.
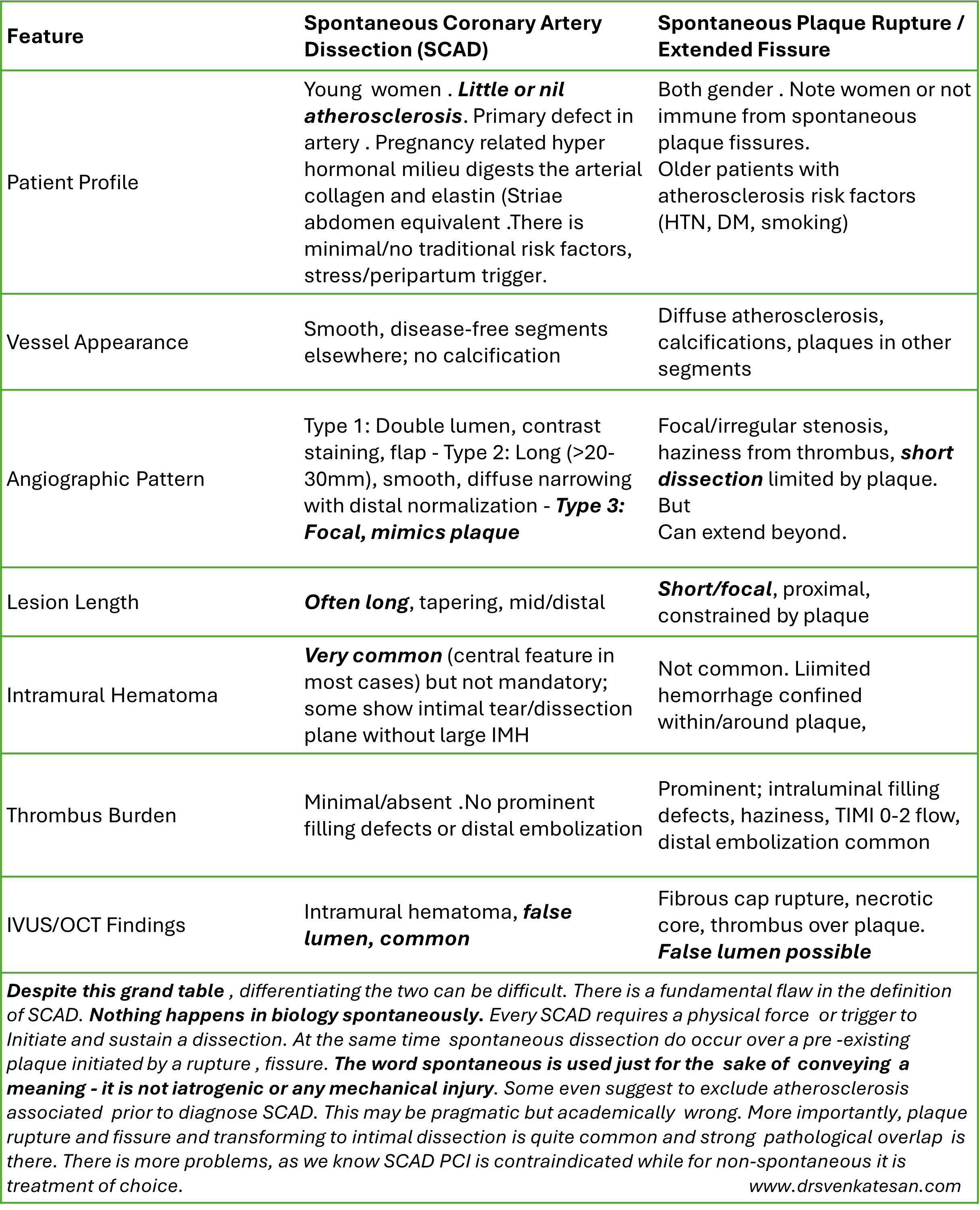
By the way, any tips to differentiate SCAD from spontaneous plaque ruptures and fissures ?
Nothing moves with out a force either from witjin or external . In both SCAD or plaque rupture , an emotional or hemodynamic stress is responsible.
The above list to differentiate SCAD from plaque fissure is big, but few are actually useful. Sometimes, the confirmation comes from the direct feel and the haptics of the lesion and the level of difficulty in crossing the lesion.
Caution : However, in explict clinical situations, as in a young pregnant women with ACS, who has a long spiral dissection , never diagnose anything other than SCAD.
Post-amble: * I wonder, how did the cardiology literature accumulated so much OCT data in SCAD, it should have been very risky procedure in those friable vessels. If PCI is contraindicated , OCT comes very close to it.
Interventricular septum, is the common shared wall between LV and RV . For various biological and hemodynamic reasons , this sharing never follows the law of equity.. It has a bias toward the bigger brother LV. Still, it never lets the RV down in contributing to RV function.
Let us see, how the IVS behaves when it comes to responding, to RV pressure overload .It is clear ,from what we know so far, IVS behavior rarely follows a pattern. We know it resists the pressure and transforms to a D shape. Does the D shaped LV really trigger an increased IVS thickness ?
IVS hypertrophy in RVH : A mixed mystery pheonmenon
In pulmonary hypertension (PHT) or any right ventricular hypertrophy (RVH), the interventricular septum (IVS) does not hypertrophy primarily due to its unique hemodynamic positioning, as IVS is anatomically and functionally linked with left ventricular (LV) mechanics. Unlike LV, the chronic RV pressure overload which is required for septal myocyte growth is rarely sustained because RV tends to dilate as well, in the process interrupting hypertrophy.
RVH occurs with elevated pulmonary artery pressures , but the pressure distibution is uneven. It is more on RV free wall and outflow tract rather than the septum. The pressure distribution concentrated at the RV free wall (infundibulum and body) .Also, the trabeculae sparing effect on IVS from direct overload .
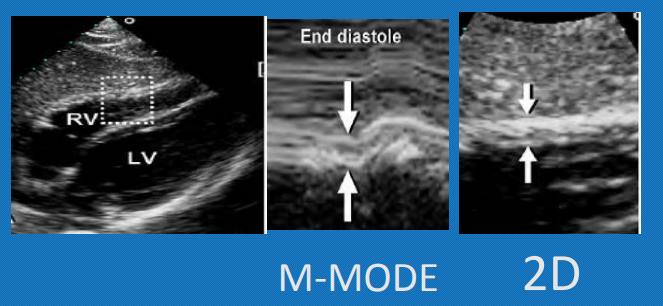
RV free wall hypertrophy defined as thickness exceeding 5 mm on echo in subcostal view in end diastole, ideally on inspiratory phase when it is maximally filled. ( MRI is a still more reliable index of RVH severity) correlating well with RV function and prognosis.
Final message
IVS rarely hypertrophies in RVH in most pathological RV pressure overload conditions. This is due to the complex shape of the RV as well as the non-uniform pressure distribution of RV intracavitary pressure. Unlike LVH, there is no strict concentric RVH. RV free wall hypertrophy is the best index for accurate identification and quantification of RVH.
A note of caution
Congenital heart diseases like isolated valvular PS, TOF can cause severe IVS hypertrophy. Similarly some Inherited or acquired infiltrative diseases can cause disproportionate RVH .We should be cautious , not to mis-classify IVS hypertrophy as LV pathology in these situations.
If any one can answer this question, correctly , he deserves some award. I am yet to find an answer.
HFpEF , by its definition has Normal EF, diastolic LV failure , LA reservoir dysfunction, combined post and pre cap PHT, with or without RV failure.
Full blown HFpEF has some what curious hemodynmics. Though we expect LA to fail in isolatiin, it is the right ventricle, that over works to tackle the elevated LAP and PH . Hence, it is likely clinical RV failure would be more common than LV.
Therorticaly, we can say , HFpEF is typical example of Bi ventricular failure as well, ie LV diastolic ,and RV systolic failure. If you want to be still more precise, it should be called triple chamber failure (LV,LA & RV)
Final message.
HFpEF continues to be complex clinical entity, with no single chamber is a primary culprit. It is a multi chamber failure. In fact, the failure initiating chamber may play lesser role than the responding chamber may react disproportionately. Please Note : LA is failure defining chamber. If it can tackle the stiff LV with all its might (compliance and contractility) , no other chamber need to fail.
Men are from Mars, women are from Venus. It may not be a fiction.afterall .It runs deep into q-bits and quark particles of our cells. The well known double X cross chromosome, epigenetics , along with hormonal interactions with cellular components make many of diseases more female centric.
Most importantly, women who are carrying a baby , are technically a chimera, and the two-way traffic of genetic materials across the placenta has unexplainable Immune interactions, making autoimmunity almost exclusively a female disorder (SLE, etc.).
Following is the partial list of women-centric heart disease
Rheumatic Heart disease: RHD is common in both genders, but it attacks the mitral valve with a strikingly different rate in females, with a ratio of up to 4:1. This difference, however, wanes with aortic valve involvement.
Mitral valve prolapse: More common in women, overriding the the fact, there are more tall men , who are likely to have more MVPS
Takotsubo (stress) cardiomyopathy: 80-90% casesoccur in women. This is surprising. (Women are known to be great fighters of stress, in all walks of life; they outlive men by 5-10 years in terms of longevity. Still, when it comes to the heart, they seem to be sensitive.)
NSTEMI vs STEMI in women(It is rather women are somewhat resistant to STEMI )
Sponatneous coronary artery dissection has well known female domnace especailluy in duiring pregnancy (estrogenic vascular elastin fracture , striae gravidourm ?)
Coronary microvascular disease: Higher prevalence in women; female rate up to 66%
Peripartum cardiomyopathy: Exclusive to women by definition, incidence 1 in 5000 live births
Heart failure with preserved ejection fraction (HFpEF): Women represent about 55-60% of cases. Odds are higher for sure. (Is that obesity ?)
Primary pulmonary hypertension (Pre -capillary , again hormonal-endothelial interaction ?)
Takayasu arteritis (aorto-arteritis): Strikingly high. Female to male ratio approximately 7:1
Mitral annular calcification: Female to male ratio roughly 2:1; more severe in women, especially elderly (Aortic annulus , males dominate )
In congenital heart disease Atrial septal defect has a female to male ratio approximately 2:1 (To remind TGA is strikingly a male disease)
Missing entities , may be added by readers
Final message
Knowing the gender difference in heart disease may not matter much, if we look at things superficially. Decades down the line, It has a huge potential in preventive cardiology, as the current genome-level interventions and female-specific vaccines might be in the offing.
News: 80% of investigations Doctors do, every day is done to satisfy, theself, the science, the patients , the peers & the hospitals or just to label a symptom complex into a disease.Just 20% help us in arrive at a diagnosis. The Irony is, it is not dificult to seperate these two categories. In fact, most of us are very much aware of junk component.
Further bit of a news : 90% of global cost of medicine is spent in prolonging the final 30 days of life of our beloved patients.
Final message
When we enter the medical school as young doctors we were taught that “Principles of practice of medicine dictates , we should always strive hard ,every moment, for an accurate diagnosis before we start the treatment for our patients” Now , after four decades into the profession , something is haunting, and trying to un-do this foundational lesson in medicine.
Post-amble
What a nonsense statement ? Do you want the modern medicine to go back to medieval times?
One of the intensively discussed, but casually taken concepts among the interventional cardiology community is to decide, when to do PCI in a non-culprit vessel in STEMI ? It is more of desire driven, rather than data driven Interventions. ( To fulfill the grandeur- mirage of complete revascularization , which occurs only in lab models )
The pendulum is swinging continuously from immediate multi-vessel PCI to delayed, deferred, (how much or as you like?) The problem is. these pendulums can be set into motion, as we desire , by different stake holders and publish them too in major journals like NEJM, Lancet, etc. The COMPLETE-NESS of evidence is mostly In-complete, if we scrutinse it properly.
Prolonging our playtime in an ACS ridden coronary artery, with a multivessel PCI can be really problematic. Every experienced cardiologist knows this fact. But RCTs (& some peer groups) that come from nowhere confuse them. Of course, some RCTs do give us the right lead. It is very unfortunate that many of us failed to learn an important lesson from the most remarkable trial CULPRIT-SHOCK (Ref 4) that came a few years ago. Since it tried to tie the hands of interventionists, it was not very admired. It proved that, if an ACS patient is hemodynamic shock , don’t touch the non-culprit vessels. (Only a few crazy cardiologists, could extract a vital , but non existent fact from this study. That is, if you want to destabilize a hemodynamically stable ACS/STEMI, try multivessel PCI)
Pros and cons of multivesel PCI in STEMI
Pros are plenty, as we can churn out an RCT as we wish, while the cons are reserved for pessimists, but they are not often imaginary.
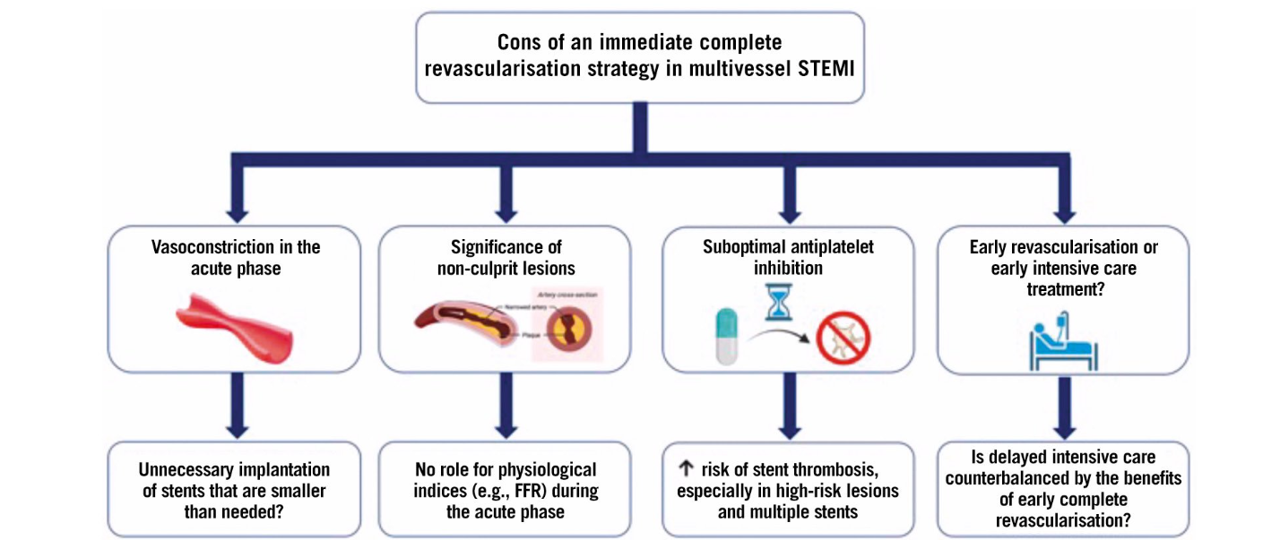
Immediate complete revascularisation after STEMI in patients with multivessel disease carries several important risks. Vasoconstriction during the acute phase may lead to unnecessary implantation of stents that are smaller than needed, potentially compromising long-term vessel patency. The assessment of non-culprit lesions is challenging in the acute setting; there is a distinct vasospastic component amplifying the lesion severity. Further there is no role for physiological indices like FFR to guide treatment, raising the possibility of unnecessary or inappropriate interventions.
Other significant concerns include suboptimal antiplatelet inhibition, which elevates the risk of stent thrombosis, especially in cases with high-risk lesions and multiple stents.
Finally, the decision to pursue early complete revascularization versus prioritizing intensive CCU care can be complex. A cath lab-centric thought process continuously interferes and clouds our intellect and common sense succumbs, i.e., an injured myocardium needs some rest after all, as do a tired cardiologist.
Final message
Should I fix that 80% LCX or 70% PDA in an anterior STEMI?
You are the boss in your lab, what you think must be right, because it is your thought. Also, you are licensed to do whatever you want to do in your patient. But, remember this: These lesions are not real culprits as of now, unless, The RCTs you love instigate them.
The architecture of HF therapy recently went on a pillar building mode .Some are strong and evidence based , still, few of the pillars are still shaky. We know the terrain for pillar building in HFpEF is much more difficult . Now, Tirzepatide seems to be a God-made molecule. It is found to be useful in HFpEF. This study (Krüger N, et al Semaglutide and Tirzepatide in Patients With Heart Failure With Preserved Ejection Fraction. JAMA. 2025 ) is from Boston, Massachusetts, adding some credibility. Read yourself and to see whether it is really sturdy or shaky pillar.
The Gut-Heart connection
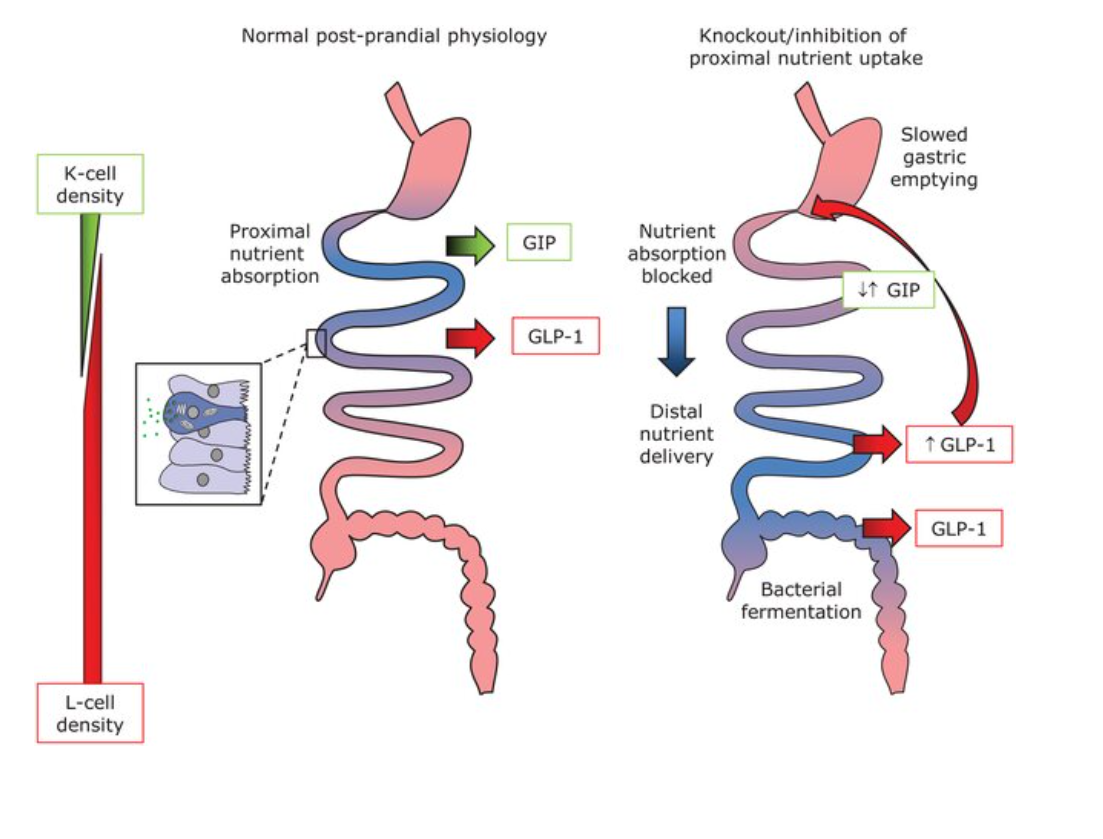
There is not much connection really. We want to connect it through Semaglutide and Tirzepatide through its antidiabetic and anti-obesity properties .How does this gut hormonal agents work in HF ? These drugs are analogues of glucagon-like peptide or gastric inhibitory polypeptide. These drugs can be called intestinal sedatives, slow down gastric emptying, reduce appetite, and hence weight loss and also diabetic control. They are secreted from K and L cells of the intestine.
Glucose dependent insulinotropic polypeptide (GIP) is secreted from K cells, which are predominantly found in the duodenum, whereas glucagon-like peptide-1 (GLP-1) is secreted from L cells, which increase in numbers in the distal intestine. Both cell types are so-called open enteroendocrine cells with direct contact to the intestinal lumen, allowing sampling of the chyme and regulate food movement and modulate insulin secretion.
Final message
Weight reduction and diabetes control are indeed vital cogs in the management of both HFrEF as well as HFpEF (more so in the latter). There are number of simple, cheap and less-glamorous ways available to reduce weight.
At any point of imagination, Tirzepatide (Mounjaro) can not claim to be an anti-cardiac failure medication. Even SGLT-2 is just a glorified glycosuric drug, stealing the credit from diuretics .
It is important to realsie, as per our past track record, the side effects of all these weight losing drugs, would knock our doors, only after a year or two.
Sometimes, someone, suddenly asks some silly question. The problem is, we don’t have much of expertise and wisdom to tell whether the question is silly or serious . The so-called sacred ratio of ideal doctor population ratio (1:1000) has come under vigorous scrutiny as the number of observational studies found little relationship between the number of doctors and the health of a society, community, district, or even a country.
This ratio was attributed to WHO, which denies , it had never recommended any such ratio. It only has some suggestions for a combined medical professionals ratio (that includes Doctors, Nurses, and paramedical professionals). We neither have split figures nor its effectiveness.
Here is some new-news in Times of India ,on the topic. It is time for all countries, planning commissions, and health regulatory bodies to do a deep introspection.
Final message
What exactly is the relationship between the doctor-population ratio and the health of a country? May be the toughest question for the entire medical profession. Meanwhile, one of my colleagues wanted to define the number of cardiologists required per unit of population for optimal cardiac care in my state of Tamil Nadu. I told him, let us sort out the basics, then we shall go for the specialist ratio.
A related article and a chat with AI to find an answer to this frivolous question.
This happened some 20 years ago. One of my senior surgical colleague casually asked a Innocuous question to me, when I was in the elevator to reach my ward. “What do you guys really mean by LV dysfunction?” When I looked at him little amused, he said…“I am asking it seriously.” My fellow mumbled to me. that this query is apparently related to the echo report, we gave, few days ago, regarding a patient with AR and severe LV dysfunction .(who is posted for AVR the next week) . I gradually realized the gravity of the situation and question.
The ambiguity is the other name for LV dysfunction
The term LV dysfunction , we use umpteen times a day, simply convey a meaning, that LV is not working well. Is that right? What is it due ? It can be simple wear and tear, fatigue, myocyte damage, ischemic or non-ischemic, myocyte necrosis, death or apoptosis. Beyond that (recall myocytes form only 33% of LV mass, the rest are something else!) Non-myocytic interstitial infiltration, fibrotic, non-fibrotic, scarring, proteo-stasis, neo-cell proliferation, chronic organized myocardial edema. Apart from this, the now outmoded terms like hibernating and stunned myocytes are also included in that LV dysfunction basket.(Finally, don’t forget about hemodynamic afterload mismatch & dysfunctional diastology )
My surgeon friend was right after all. Which LV dysfunction are we talking about? Learned a harsh lesson. Our academic ignorance is explicit, still going around the wards majestically. Realised as a cardiologist we have the responsibility to find , (or at least make an effort) the various components of LV dysfunction.
Mechanism of LV Dysfunction in AS vs AR
Differences in Mechanism
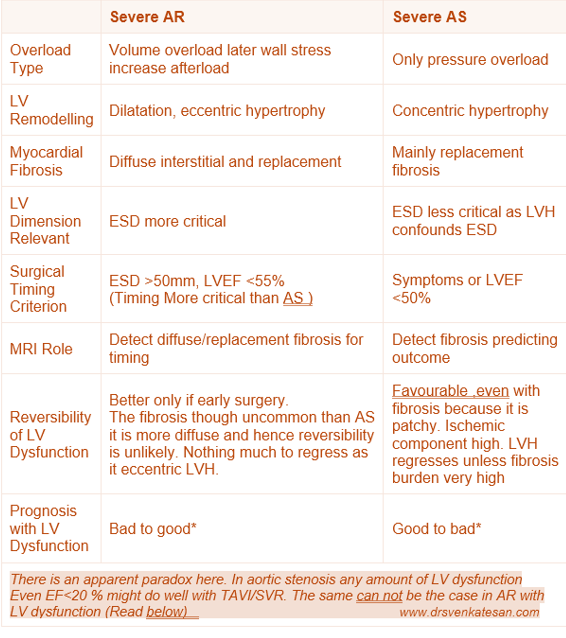
AR involves volume overload with LV dilation and eccentric hypertrophy with diffuse myocardial fibrosis. AS involves pressure overload with concentric hypertrophy and more focal replacement fibrosis. Both conditions lead to fibrosis, but the pattern, timing, and extent vary.
Clinical Implications in Timing of Surgery
Surgery in severe AR should be considered before irreversible LV dysfunction, guided by indexed LV dimensions (especially end-systolic diameter >50 mm or indexed >25 mm/m²), or LVEF <55%. Waiting too long allows fibrosis and remodeling to reduce recovery chances. In severe AS, surgery is indicated once symptoms develop or LV ejection fraction falls below 50%.
Role of LV Dimensions EDD and ESD
LV End-Diastolic Diameter (EDD): Reflects volume status and remodeling, important for AR where volume overload is predominant.It is less useful as it is pre-load dependent.
LV End-Systolic Diameter (ESD): ESD is unique parameter as it represent a topmost point ( north west) in cardiac pressure volume loop , when the contractility is load independent . it is a strong predictor of contractile function and prognosis.
Role of Cardiac MRI in Identifying Reversible LV Dysfunction
Role of MRI is vital. Cardiac MRI uses late gadolinium enhancement (LGE) to detect replacement fibrosis (scar) and T1 mapping/extracellular volume (ECV) quantification to detect diffuse interstitial fibrosis. *LGE: Late mean 20 minutes , the tissue stagnates and fails to get wash off and appear enhanced
Reversibility of LV Dysfunction in AS & AR : Is there a paradox ?
Patients with severe AR generally exhibit better reversibility and prognosis post-surgery compared to those with AS, (Ref 7 : This study found patients AR tend to have more diffuse fibrosis, which exhibits better regression after valve surgery compared to the focal replacement fibrosis in pressure overload conditions (like AS). This suggests better reversibility of LV dysfunction in AR) This finding is an apparent paradox, since we think LVH is more likely to have fibrosis.
Timing of surgery is more critical in AS or AR ?
Patients with severe AS and very low LVEF can still experience significant improvement in LV function and survival after AVR.
The explanation is that in AS, the primary problem is a mechanical pressure overload due to valve obstruction. AVR abruptly relieves the afterload, decreasing LV wall stress, and allowing recovery of myocardial function, sometimes dramatically.
Even patients with severely reduced systolic function can see meaningful functional recovery post-AVR if myocardial fibrosis and irreversible damage are not advanced.
AR Patients with Moderate or Low EF After AVR
In contrast, patients with AR who have even moderate reductions in LVEF tend to have worse outcomes post-surgery.
The explanation lies in the gradual volume overload and progressive LV dilation in AR, leading to more diffuse myocardial remodeling and fibrosis that may be less reversible.
The reduction in afterload after surgery in AR is more gradual and less dramatic than in AS, and by the time EF is moderately reduced, irreversible myocardial damage often limits recovery.
Thus, surgery is ideally timed much earlier in AR (before moderate EF decline) to optimize
The non-forbidden question
Why should we wait? Is time a muscle only in ACS? Not in valvular heart disease? Can’t we intervene in all patients with severe AS/AR irrespective of LV function before it worsens?
Yes, time is indeed muscle even in VHD. This concept looks attractive. Many centers follow this, ignoring the current guidelines. (The issue here is dependence on artificial valves for the rest of life and the attendant risks.)
Final message
It is indeed true, cardiologists use the term LV dysfunction so commonly and casually, without elaborating on its true meaning. Whenever and wherever possible, we must take efforts to list and quantify various components of LV dysfunction, and also the likelihood of reversibility.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.