No doctor will want any disease to progress in their patients. But, coronary revascularization is an enigma. Cardiologists take every step to regress the atherosclerotic process and be meticulous in maintaining antegrade flow across the left main and proximal LAD or LCX. They double up their caution after PCI in left main or proximal segments.
Meanwhile, our cardiac surgeons do enjoy a unique liberty. In fact it is a luxury, i.e., they can afford to forget the status of proximal disease. What they want is the patency of the graft, integrity of the anastomotic site, and distal vessel status. Atherosclerosis being essentially a proximal disease, surgeons have all the more reason to be blessed. Of course, it should have been disciplined well-done CABG.
Do they ever wish for proximal vessel disease progression ?
What a non-sensical question, dude ?. Don’t get shocked. I was told, many of surgeons would, indeed be happy with that, as it tends to divert more flow to the graft, and long term patency is better. There are many instances when they close the antegrade flow, if it is interfering with graft flow during the surgery itself. .
Final message
Cardiologists strive hard to heal at ground zero where vessels are traumatized. Worrying day in and day out, after putting a scaffold. Surgeons simply fly over it, laughing at the lesions. So, what is the lesson from this post? When making critical decisions on coronary revascularization, think twice .Make a learned decision for every given patient.
Counterpoint
Native vessel progression do have adverse outcomes even after CABG, provided it occurs in the non by-passed vessel or when it occurs distal to the bypass circuit. Please ,don’t take a wrong message that progression of atherosclerosis is welcome post CABG. Every post-CABG patient should follow the same OMT and lifestyle modifications to reduce the burden of atherosclerosis in a larger sense. What this article refers to, is mainly about the influence of disproportionately high antegrade flow on graft survival. Surgeons do prescribe statin after CABG routinely , not withstanding the results of ACTIVE study (Ref 2) which showed high Intensity statin following CABG, had little influence on graft patency.
Dyspnea is one of the commonest symptoms in medical practice. Whatever be the trigger, ultimately, it is a sensory perception, felt at the level of the cortex (to be specific, the Amygdala nucleus) decides the intensity . The initiating receptor usually arises from the muscle spindles , due to mismatch in the length and tension . These spindles are located widespread in intercostal and other respiratory muscles. The afferent pathways are complex, as are the brain stem processing centers and cortical modifications—all matters.
(* A proposed definition with mechanism :Both physiological and pathological dyspnea are the unpleasant breathing awareness (In time), till for the oxygen debt is repaid to the depleted mitochondrial, ATP treasury , for the cost of excess respiratory work done, is one popular definition )
The complexity of the neural circuit for dyspnea can be judged, even if the cranial or spinal pathways i.e., vagus or spinal transection, dyspnea is not fully relieved (experiments on post-vagotomy, quadriplegic patients, and transverse myelitis). The answer might look simple in one way. Please mind, we don’t need an intact nervous system to carry afferent dyspnea signals to the brain centers. It can simply be carried by blood, to the central chemoreceptor in biochemical form.
The uniqueness of this symptom is , it can be entirely physiological , or a harbinger of Instant fatality as in acute pulmonary embolism or LVF. Resting dyspnea is always a concern, unlike exertional which has more benign cause. As a cardiologist, we always equate dyspnea to elevated LVEDP and possible LVF . Though RV failure can also cause dyspnea.
Generally, young fellows might ignore non -cardiac non- pulmonary cause of dyspnea. It is better to reemphasize ,the commonest cause of dyspnea missed in ERs and ICUs are metabolic or systemic in nature . (We have seen Kusmaul’s breathing of DKA raising false cardiac alarm )
Systemic causes of dyspnea (With normal PCWP)
Metabolic dyspnea*
Bio-chemical dyspnea*
Anemia*
Most lung diseases
*Chemo receptors are as important as baro- recptors of heart and J receptors in lungs
Is cardiac dyspnea possible with normal PCWP ?
Pre capillary Pulmonary HT (Isolated Arterial PH)
RV infarction.
Classical Hypoxic dyspnes in cyanotic heart disease (TOF,)
Any RV failure , can trigger RV baro-receptors(similar to LV but less concentrated)
Final message
Dyspnea: is it from the heart or lungs? This popular debate has been going on for decades and was answered in a landmark review published four decades ago.(JAMA 1982).Every one of us, must go through this to understand critical cause of dyspnea that arise from heart and lungs.
However, if the question is, which is the commonest cause for exertional dyspnea? Is it from the heart or lungs? The answer is neither of the two. The commonest cause of dyspnea as a whole is neither from the heart nor lungs. It is probably anemia, physical deconditioning, fragility, or sluggish systemic skeletal muscle respiratory status due to a sedentary lifestyle. This explains why a marathon runner can run 42 km without stopping, while a healthy middle-aged man struggles to climb even three floors because of sedentary activity.
Paclitaxel: Is a highly lipophilic, and rapidly absorbed by vessel walls and retained for days to weeks, making it ideal for DEBs, which deliver the drug during brief balloon inflation (30–60 seconds). Its cytotoxic action, disrupting microtubules and arresting cells in the M-phase, effectively inhibits neointimal hyperplasia without requiring prolonged drug release.
Sirolimus: Less lipophilic, sirolimus requires sustained release to achieve therapeutic levels, as it acts cytostatically by inhibiting the mTOR pathway, arresting cells in the G1 phase. This suits DESs, which provide continuous drug elution over weeks via polymer coatings. Its lower tissue retention makes it less effective for short-contact DEBs.
Paclitaxel hurts the endothelium with DES, but it heals with DEB ? How is this possible ?
Paclitaxel’s association with delayed healing and inflammation raised concerns about long-term safety in DESs, particularly after reports of late and very late stent thrombosis. It is abandoned in DES platform.
Paclitaxel born again as DEB avatar
It is claimed, Paclitaxel’s rapid uptake and lipophilicity make it suitable for DEBs, while sirolimus’s need for sustained release and favorable long-term profile suits DESs. It is very hard to believe, the published evidence, however robust they are. Only thing I can guess is, Paclitaxel enjoys a safety net in DEB , as the drug disappears so quickly before any useful effect or side effect could manifest. Ongoing research into sirolimus-coated balloons may shift this paradigm. Till then, we have to trust Paclitaxel, that remains the standard for DEBs due to pure scientific reasons.
Final message
Paclitaxel, which was at its crowning glory during the SYNTAX times , was phased out in DES due to various/ serious untoward effects.
Please bear with this highly biased opinion. I suspect, as a face-saving measure, the industry accommodated Paclitaxel into the DEB platform when it was chucked out of DES. I think we must learn to find truthful pathways of research.
Understanding sympathetic nervous had never been easy. (It doesn’t in any way mean, we have mastered para-sympathetic !). As physicians and cardiologists, we are expected to know the updated adrenergic, dopaminergic, imidazoline receptors etc. We need to know at-least an overview of its current nomenclature, area of distribution, benefits of blocking and stimulating them. Unfortunately, many of us consider it as student stuff and too theoretical for a busy cardiologist.
A realistic scenerio
Then one fine day, an I-pad wielding ,medical representative would come, late in night and teach us about a new drug called Moxonidine. “Sir this is a combined alpha and Imidazoline-1 agonist. Just .2 mg is enough sir to treat any refractory HT” We nod our heads sheepishly, wondering what is that Imidazoline ? Why is this guy is saying alpha agonist* ?
*So far I had been thinking only alpha blockers, have anti-hypertensive action. It took few moments to make some sense . Oh, okay, I got it, Clonidine and Prazosin are entirely different groups of drugs, though they act on alpha receptors—one stimulating and other blocking at different sites.
This post is meant to avoid such embarrassing situations.
Final message
Let us learn new things every day , but never think, reviewing what we read in the past is a mean academic activity.
PPCM is a rare but an Important cardiac condition, that contribute to significant maternal and fetal morbidity and mortality.So many variables , triggers, back ground risks have been studied for decoding the pathogenesis of PPCM.
Does the sex of baby inside the mothers womb, in any way influence the incidence of PPCM ?
When searched in the literarure, I found almost no data on this simple parameter. While there is a lot of reference for PPCM relationships in twins and multigravida, none looked at gender specifically. From personal discussions with my Obstetrician colleagues, few suggested female babies are often seen to precipitate PPCM . I think it is an academic oversight, that we haven’t looked at the gender angle as yet, for this important entity.
Is there really no evidence ?
Yes, it is sursprisngly true . Gender as a variable may have been overlooked because it hasn’t shown up as a signal in preliminary data . Researchers often rely on patterns in existing data to guide hypotheses, and if no pattern suggests fetal gender matters, it may not be pursued. In some studies, gender data might be collected but not analyzed or reported.
It is a fertile research field. It may look like a simple study, but it can throw more light on this mystery myocardial disease that is directly related to pregnancy.
Could Fetal Gender Be Relevant in PPCM ?
While no evidence currently supports a link, there are theoretical reasons why fetal gender could be important.
Placental Differences: We know male and female fetuses have slightly different placental gene expression and responses to maternal stress, which could theoretically influence maternal cardiovascular load or immune responses.
Microchimerism: If fetal cells contribute to PPCM via immune mechanisms, sex-specific differences in cell behavior (e.g., Y-chromosome-related antigens) could be explored.( though this is speculative)
Hormonal Influence: Fetal sex might influence maternal hormonal profiles (e.g., via placental hormones), Female fetus are known to have more intense estrogenic effect in maternal circualtion.
Pregnancies with female fetuses may be associated with slightly higher levels of hCG or placental aromatase activity, which could theoretically enhance estrogen production or mimic an estrogenic effect in some contexts.(Ref 3)
What are the maternal diseases that are shown to be correlated with fetal sex ? (Ref 1, & 2)
Some maternal diseases, such as preeclampsia, gestational diabetes, preterm birth, hyperemesis gravidarum, autoimmune diseases, and asthma, have been associated with fetal gender in limited studies, with male fetuses often linked to slightly higher risks for preeclampsia and GDM, andfemale fetuses to hyperemesis and asthma exacerbations. However, these correlations are generally weak, and mechanisms are not fully understood. For PPCM, no evidence exists
Final message
Fetal gender is a simple, routinely collected variable, making it feasible to include in future studies without significant cost. If even a small association exists, it could refine risk stratification or guide mechanistic research (e.g., exploring sex-specific placental factors). The lack of data on this parameter represents a knowledge deficit in cardio obsterics that could be addressed in large registries or meta-analyses, especially as PPCM research has grown significantly in recent times.
*Request the fellows in O&G and cardiology to conduct a specific study on this topic and enrich the literature on PPCM. I think the data is already there in every PPCM paper. We just need to collate. (There is no copyright for this topic, but please acknowledge, if no one has done this aspect of a study in PPCM before)
The answer is, yes, but a crude yes. A lot of OCT literature has taken this aspect casually. Macrophages, both resident and blood borne monocyte-macrophage, lay the foundation for the athersclerotic plaques. Currently, cardiology imaging specialists tell us, that bright spots in OCT, beneath the Intima are believed to be macrophages, based on a few histological correlation studies. If you go through these studies (Ref 1), it is almost guessing like tossing a coin .It finds 57% of bright spots were macrophages. The rest 43 % can be any of the following 7 in the list.
The causes of bright spots in OCT are too many
1.Lipid Pools/Necrotic Core: Lipid-rich areas or necrotic cores in plaques can appear as hyperreflective spots.These may mimic macrophage infiltration but are typically larger and less discrete.
2.Cholesterol Crystals: Resemble macrophage-related foci but are often linear or needle-like.
3.Calcifications: We know calcium is always a bright spotin any Imaging. Same with OCT Microcalcifications or early calcium deposits in plaques can appear as bright easily mistake formacrophage. But, unlike macrophages, calcifications are often accompanied by acoustic shadowing.
4.Fibrous Tissue: Dense fibrous tissue in stable plaques may occasionally produce bright spots, particularly if imaging artifacts enhance their reflectivity.
5.Neovascularization: Reflection due to red blood cell content or vessel wall components, mimick macrophage accumulation.
6.Thrombus: Small thrombi (red or white) within plaques can appear as bright spots.
7.Imaging Artifacts: Motion artifacts, stent strut reflections, or incomplete blood clearing during OCT imaging can produce spurious hyperreflective spots that mimic macrophages.
Please note :The most important factor in the above list, is the last one, ie technical and Imaging artifact.
Can we identify true macrohoages with emerging technologies ?
We are in the era of virtual histology. It may come true in the future. Current generation OCTs have 10 to 20 micron resolution.
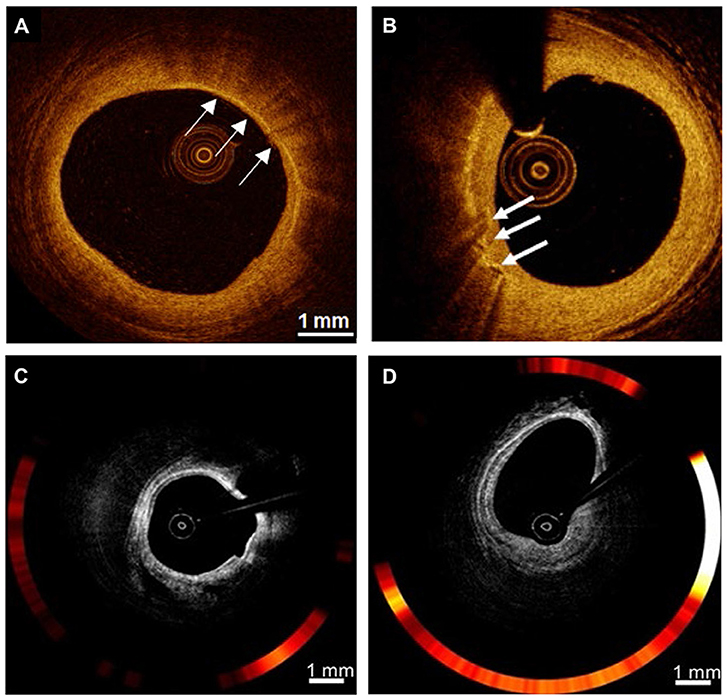
Image source (Ref 2)OCT cross-section images of the atherosclerotic vessel lumen, the location indicated by the white arrow is, rather susspected the macrophage. (C,D)
Advanced techniques like USPIO*-enhanced OCT and μOCT** show promise for more precise macrophage detection, but they are not yet standard in clinical practice. For now, OCT remains a valuable tool for assessing plaque vulnerability, in which we believe macrophages are playing a key trigger.
What is purpose of identifying these macrophages with such costly technology?
Not much really. May be a feel of scientific enthrallment. Of course, it can help monitor plaque healing, which is going to happen anyway whether we visulaize it or not if proper medications are taken (Intensive dose statin). Ofcoure ,these imaging modes do have a role , if we want to know how the macrophages are going to feed on the bio-absorbable stents.
Final message
All that blinks bright in OCT, are not macrophages. Virtual histology-based interventions are great scientific tools, but have little value in cath lab interventions as of now.
The answer is an unequivocal yes. The catch is, DES , tends to whip out the macrophages from its vicinty . BMS welcomes it . Which is good ? Think about it , answer will be very surprising.
I am neither an active or inactive Interventional cardiologist. But, I have sat through numerous sessions of complex PCI workshops. I used to wonder why they give so much importance to the side branch crossing. Obviously, it must be for some good reason. I did this brief write-up, trying to comprehend some sense. Hope the experts would agree with this.
This study looked into the clinical characters of STEMI presentation and correlated with various aspects including Troponin levels with reference tothe clinical factors.
Reproducing just one sample data about the character of chest pain. Please go through the complete paper.
Few observations need a comment
The pull or catchining type of pain has 0% likelyhood of STEMI.The last in the list is mentioned as dyspnea is of great importance.It is the angina equivalnet ,which is reported to be 50 % is quiet high.
One observation, and an unlikely miss I could found, is the incidence of epigastric pain and rare abdominal pain in some of those pateints with inferio posterior MI where it direct intimacy with diaphgram and whcih can radiate downwrds.We have missed some cases as acute abdomen, as pancreatitis , later on proven to be RCA STEMI.
Final message
We keep talking at length, dozens of listless trials fighting between single or two stent strategies in bifurcation lesions in every compulsive interventional workshop. Currently, I don’t think any conference would give a stage space to discuss trials such as TRAP-AMI which can infuse fresh thoughts in youngsters’ minds. It is an unrealistic wish though; any cardiology scientific committee should be mandatorily instructed to allot at least 30% of time to clinical cardiology that can bring back the field of cardiology, on the righteous track again.
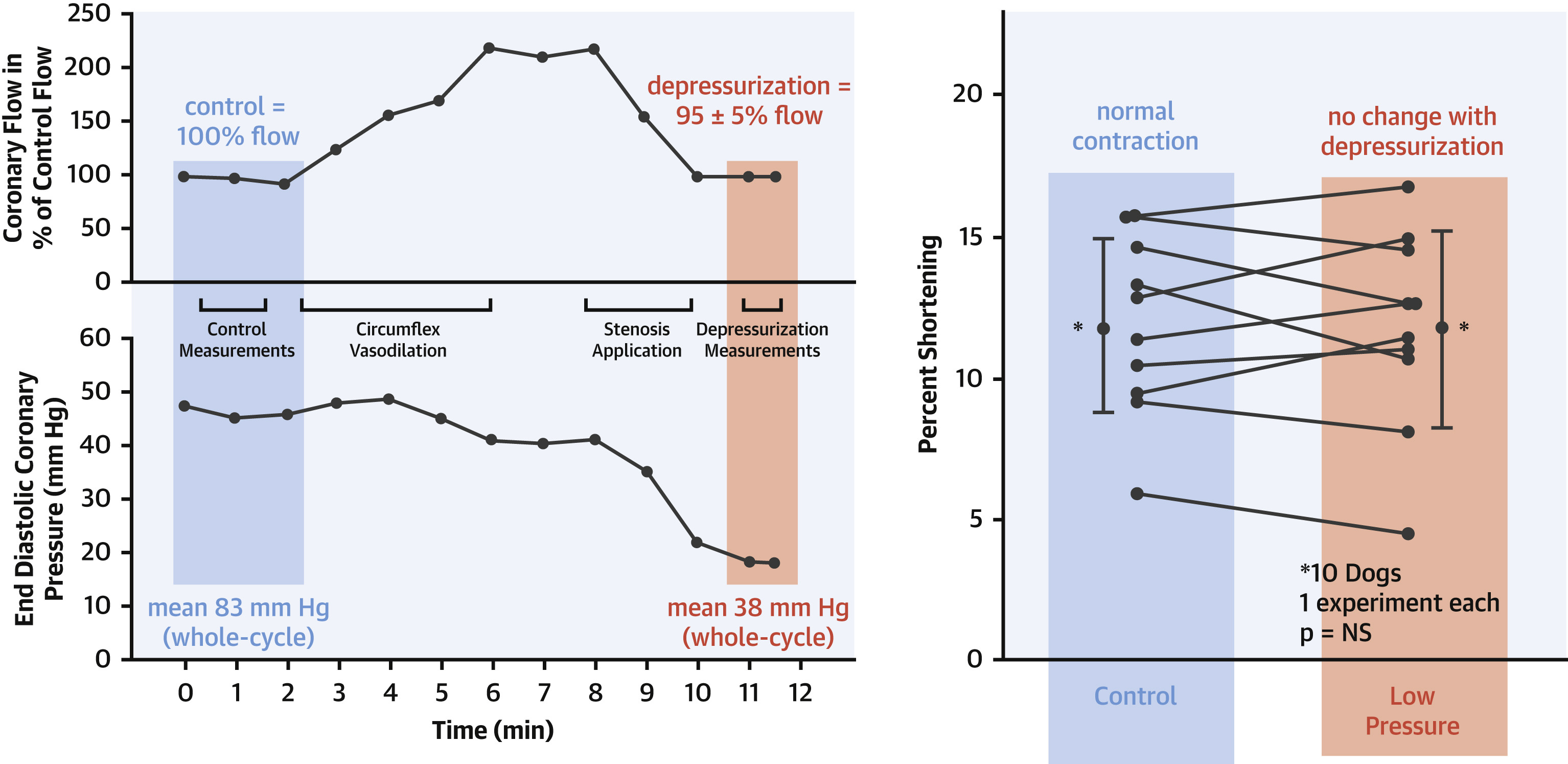
1.Is systemic HT an advantage ?so that high pressure head aids in pushing the blood across the lesion. ?
I don’t know whether I can say Yes*, physiologically, the high proximal pressure and low distal pressure help maintain the flow. The distal drop happens due to the tightness of the lesion itself, but that is counterproductive, unless tone of the distal microvascular bed is intact and dilates fully.
*Mind you, IABP during cardiogenic shock, essentially does this – keep the coroanry diastolic pressure high.
However, there are significant caveats.
There is law of diminishing Returns : In a 90% lesion, the resistance is so high that even elevated Pa may not substantially increase flow due to the fixed obstruction. Hypertension increases left ventricular afterload, raising myocardial oxygen demand. In a 90% LAD lesion with compromised flow, this can worsen ischemia, outweighing any flow benefit from higher pressure.
2.What happens to trans-lesion flow during hypotension ?
This has direct implications when a patient with a significant lesion develops hypotension due to a systemic cause like dehydration or postoperative hypovolemia. We have often observed transient ST/T changes in a postoperative patient that may or may not lead to full-blown ACS.
To know what exactly happens across a lesion, we need to understand coronary autoregulation and its limits. Coronary autoregulation maintains stable myocardial blood flow despite changes in coronary perfusion pressure. Its limits and range are as follows. .
Range of Autoregulation: In healthy coronary arteries, autoregulation operates effectively between perfusion pressures of approximately 50–60 mmHg to 120–140 mmHg. Within this range, vascular smooth muscle in coronary arterioles adjusts resistance to maintain near-constant blood flow.Lower Limit: Below 50–60 mmHg, autoregulation fails, and blood flow becomes pressure-dependent. This can lead to ischemia, especially in the subendocardium, which is most vulnerable due to higher oxygen demand.Upper Limit: Above 120–140 mmHg, maximal vasodilation is reached, and further increases in pressure do not significantly increase flow.
However , we don’t know how this autoregulatory biological servo control, is tampered in the presence of a single or a tandem lesions.
3.How does FFR gets altered during exertion in such lesion ?
We have very limited data available on this and are essentially ignorant . FFR during exertion typically decreases compared to rest due to the amplified pressure gradient across the stenosis driven by increased flow demand and limited reserve.However collaterals can mitigate this fall in FFR.
Final message
Putting a stent across 90% lesion surely is a childish task, when compared to understanding complex hemodynamic vortices that happen across it.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.