If you think this quote is too brutal, please visit the Nobel laureate Initiative “Lown Institute” website and spend some time, to find solutions to rescue the medical profession, which is rapidly drowning in a sea of ethical dysfunction.
If you think this quote is too brutal, please visit the Nobel laureate Initiative “Lown Institute” website and spend some time, to find solutions to rescue the medical profession, which is rapidly drowning in a sea of ethical dysfunction.
Posted in Uncategorized |
A simple question with mammoth repercussions in the revascularization world.
How was the question ? Was it difficult ?
Don’t worry, it wouldn’t be the same even for elite cardiology experts worldwide. It is not a Himalayan task, though, to find an answer. All it requires is a simple FFR run through pre and post PCI (Now RFR, iFR, QFR). Surprisingly, very few inquisitive minds wanted to do this. I can find 5 related papers. The fifth one is very specific: REPEAT-FFR study. Go through at least that one paper and find the answer yourself.
Cardiology fellows it is worth reading about this important study , might be asked in exams.

Final message
The conclusions from these studies are not really baffling, but demand a lot of academic cleansing of our understanding about the relationship between epicardial patency and microvascular flow.”It is obvious from these studies that epicardial PCI never guarantees good revascularization with a FFR backing “
Every cardiologist should ask this question before they scrub, whether the PCI, they are going to do today, would improve the net-myocardial flow, LV function or symptoms . Are we doing justice to our patient (or blindly practicing science) who is quietly lying on the table, with a mix of anxiety and trust, with a complete belief that what they are undergoing is a life-changing or life-saving procedure.
Further, it is our duty to restore the lost glory to the defamed , stigmatised medical management of CAD & Impress our patients that “All that, doesn’t glitter could be pure gold as well”
Reference
For those people who are too busy to click on the link .Summary of REPEAT-FFR study .

Posted in Uncategorized | Tagged acc aha, bari 2 d, courage study, eapci, epicardial myocardial dissociiation, es guideinnedmt, ffr, ffr rfr qfr, ffr vs oct, ISCHEMIA trial, medical management for cad, myocardial revascularisation, ORBITA study |
No medical painting Impacted us this much. “The Doctor“ “was exhibited in 1891 by Sir Luke Fildes and Presented by Sir Henry Tate in 1894 in London. I am sure most of us are aware of this painting. Sharing it for future generations. Wish, this painting is embedded permanently in every young medico’s nimble brain.
This painting soulfully pours the silent and sacred bond between a helpless doctor and his dying patient, , which happens to be a lovely child.
Further reading: https://www.tate.org.uk/art/artworks/fildes-the-doctor-n01522
Posted in Uncategorized |
Anyone who is flushed with millions can become a member of “The Hurlinghamin” London or the “Yacht” in Monaco, or any other glamorous clubs in the world. But, EBC* is different. Only cardiologists are privileged to enter. EBC is obviously unique. It is the only club addressing exclusively a subset CAD, ie bifurcation coronary lesions. Apart from immense pride and academic entertainment, it teaches us some deep technical points. (By the way, BFL* is a minuscule spoke in the gigantic wheels of global atherosclerosis)
Approach to BFL
90% of BFL still require only drugs or humble single stent or a provisional second stent strategy. However, as per basic rules of human intellect, lesser problems continue to bother us and consume our precise time. This continues, even after realisng , there are 6 complex two stent strategies that doubles up complications.
(*EBC -European Bifurcation club .BFL-Bifurcation lesion)
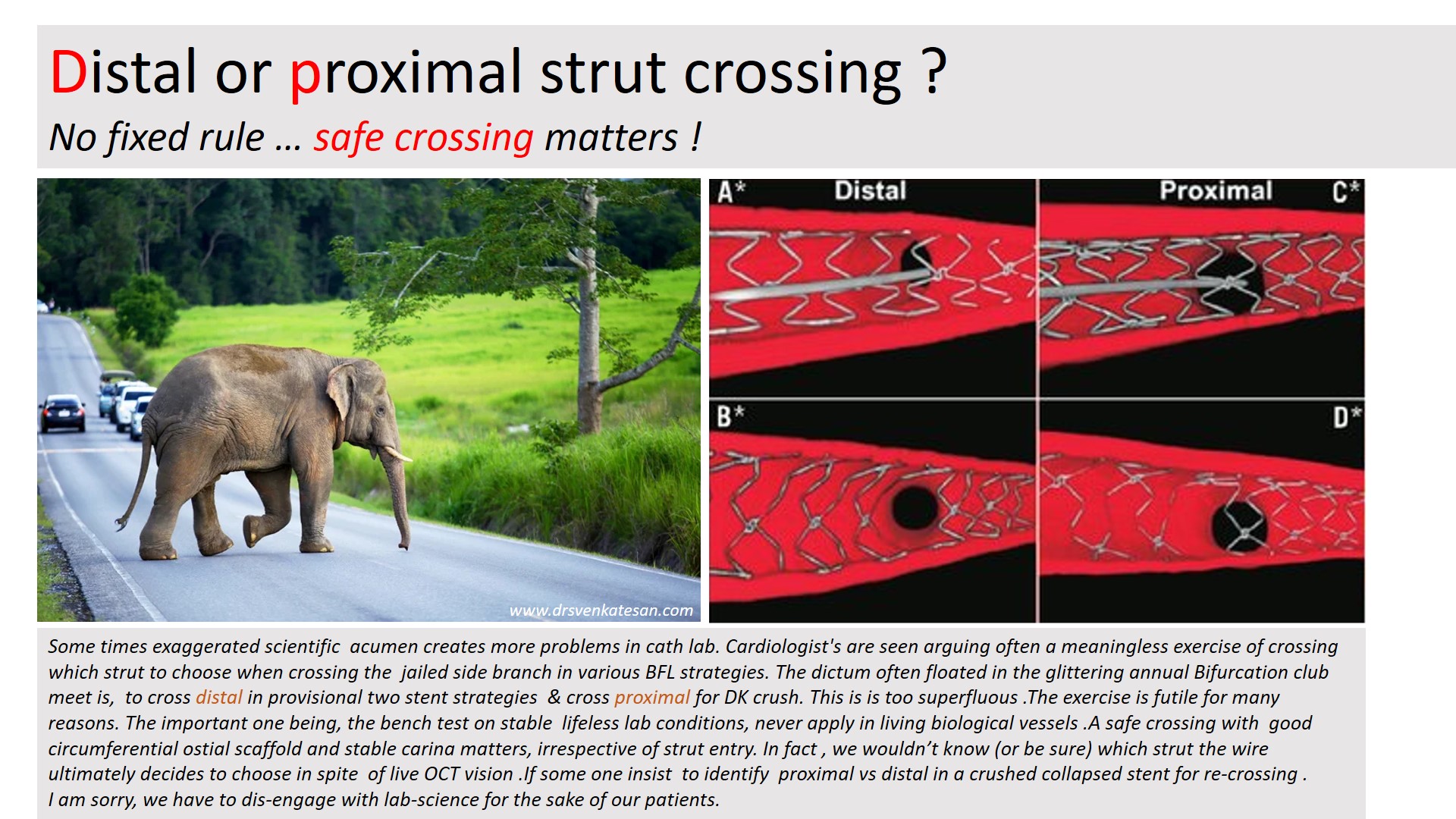
We will address one unique issue in BFL. May not be a major clinical issue .Still, it’s worth it. It is about the side branch crossing after the intentional jailing of the side branch.
Let us answer this query first
Pure science: Observations from Bench test (Text from Ref 1)
In contrast to provisional stenting in which re-crossing through a distal strut is desirable, initial re-crossing the crushed SB stent in the DK crush technique should be done through a proximal stent strut to minimise the risk of SB stent deformation. A theoretical exception could include bifurcations with a particularly narrow angle for which proximal re-crossing may shift more struts towards the MV, leading to a less desirable, longer neocarina. The 2nd recrossing should be done through a distal strut.
Bench testing is clear. Still , Why this confusion ?
We are all talking about theory in bench testing in stable non-hemodynamic conditions that lacks a biological carina and the dynamics of plaques. We are aware that there are at least 5 virtual ostia in every bifurcation arena (or trifurcation) . The qunatum and direction of plaque sharing occurs with a random effect. We also know the final kissing either cements these plaques perfectly or unsettles in a most bizarre way. So, these strut crossing stuff, are more of an imaginary bio-engineering principles. Whichever strut you cross, do it slowly, gently dilate it to the maximum within the polygonal confluence and good approximation. Don’t get too much carried away , even live online OCT guidance do not guarantee a perfect crossing.
Final message
The answer to the title question seems to be (me), one need not hair-split much on the site of crossing at the side branch. Fortunately, in whatever way, we weave the metallic mesh*, at the epicenter of the coronary highway, it is the natural secretagogues like TPa, Nitric oxide, PGI-2, along with DAPT decides the patient’s genomic fate.
*An appeal to all EBC club members.Before embarking upon a compex PCI on a stable patient , please think for one last time , whether your patient might do well, only with medicines.
Referecne
1.Hall AB, Chavez I, Garcia S, Gössl M, Poulose A, Sorajja P, Wang Y, Louvard Y, Chatzizisis YS, Banerjee S, Xenogiannis I, Burke MN, Brilakis ES; Collaborators. Double kissing crush bifurcation stenting: step-by-step troubleshooting. EuroIntervention. 2021 Jul 20;17(4):e317-e325. doi: 10.4244/EIJ-D-19-00721. PMID: 32310131; PMCID: PMC8919516.
Posted in Uncategorized | Tagged bifurcation lesion, crosssing side branch, dk crush, ebc club, esc acc aha esc, jailed side branch, scai, single or two stent strategies |
AVR plus MVR commonly refered to as DVR is a path breaking cardiac surgery in patients with combined valvular heart disease. Still, it carries considerable mortabidity, if not done with high degree of expetise and standards . Apart from technical perfection, an inherent issue exist that might affect long term Impact.
Here is lateral view of X – ray chest showing a DVR.
High resolution jpeg Image

Final message
What will happen to the native anatomical and physiological functional unit of Aorto-mitral continuity after DVR? Will LV inflow encroach the LV outflow or vice versa? These questions are less often asked. In the process, we often ignore a concept called Aortic-mitral coupling or inter-dependence.
Reference
Posted in Uncategorized | Tagged aorto mitral continuity, aorto mitral coupling, commando operation in dvr, davids surgery, double valve replacement, dvr, infective endocarditis and dvr, inter valvular fibrosa, outcome after dvr, tavi vs mvr |
Stents have become essential coronary jewelry in global CAD care. The usage of these glamorous metals inside the human heart has crossed many millions, and aiming for a billion. Obviously, when used on such a large scale un-toward events are not an exception.
Stent migration
While the complication list of coronary stenting hangs long, fortunately, stent migration is a rare event. , Though, early geographical miss is common during deployment, these episodes don’t come under stent migration. Stent dislodgement during the procedure is a more common technical defect.If not recognized it may be wrongly labeled as late migration Exaggerated longitudinal shortening sometimes mimics migration.
Minor stent skids or mini migrations in cath labs are acceptable, distant and wayward migration to dangerous zones can be problematic.

True migration may be defined as a stent moving away from the target zone in the short or long term from its original location. It is useful and can be further divided with reference to time like peri procedural, short term, and late. Though it is generally thought to be rare true Incidence is not known. (Colkesen AY, . Int Heart J. 2007;48(2):129–136.)
Mechanism
It is not always easy to find the reason for migration. Many of the following factors could operate
Implication
Stent migration can be totally unrecognized by many, while could end with a dramatic clinical event depending upon the extent and location of migration.
Extraluminal migration into pericardial space has been reported. Praloy Chakraborty, J Am Coll Cardiol Case Rep. 2021 May, 3 (5) 745–746
How do we manage this?
Though it is a sort of crisis for cardiologists, very often patients are asymptomatic and comfortable in spite of migration. (After all, it is the same pro-thrombotic foreign body even if it is present in its original place, is it not ?) Minor migration or embolization to safe zones need not require any intervention.
What should we do if leaving alone is not an option?
Crossing the stent and deploying it again or trapping or crushing it with another stent or retrieval are various options. Surgery is the last resort if the migrated stent is compromising blood flow critically.
Stent migration: A mini ethical crisis
Should we inform the patient about this adverse event?
Never hide any info from your patient about his or her health. It may amount to serious negligence. Sorry, I beg to differ*. If we really feel, it is a safe migration, and if the patient’s (& relatives) anxiety is too high, principles of practice of medicine can be selectively put on hold, for the overall benefit of the patient. (Of course, legal requirements are to be fulfilled by documenting the event in a complex manner as the lawyers do )
*Once you inform the patient, the option of leaving it unattended is a Herculean task even if it’s benign migration. (at least in our country) We have had long debates about this. Once upon a time, we had a stent that got dislodged and lost in circulation, and after long times of screening, there was a suggestion of a stent in the pelvic branches of the iliac artery. I will leave to your imagination, what we did for that patient.
Final message
Stents have conquered our profession and it is a life-sustaining device for both patients and cardiologists. Along with it, we have percutaneous valves, wires ,plugs, disc conduits, ICDs etc, Welcome to the big world of vascular foreign bodies. We are supposed to get optimally trained to keep all this stuff within the circulatory system smoothly running. If you look in that perspective, stent migration may be considered a minuscule untoward event. This doesn’t mean we can take this entity casually. We need to be familiar with its true incidence, mechanisms, potential solutions, and preventive strategies.
Reference

1.Bews and others, Coronary stent on the move, European Heart Journal – Case Reports, Volume 5, Issue 12, December 2021, ytab511, https://doi.org/10.1093/ehjcr/ytab511
2.Kasegaonkar AM, Chudgar P, Kamat N, Burkule N, Dhareshwar J, Dalal A. Delayed Presentation of Intracoronary Stent Migration in Pericardial Space: Role of Imaging. Indian Journal of Clinical Cardiology. 2022;3(4):209-210. doi:10.1177/26324636221087108
Posted in Uncategorized | Tagged stent migration |
It is year 2009.
A 16 year old boy presented with Anginal pain.
I think this child underwent successful surgical correction.
What is the mechanism of angina in coronary AV fistula ?
Coronary steal is easy explanation. But, very few of them develop functional Ischemia even at exertion. Why ? Size of fistula. dainage site, complex tortuous tracts, associated microvascular obstruction, contribute more.
Reference
Angelini P. Functionally significant versus intriguingly different coronary artery anatomy: anatomo-clinical correlations in coronary anomalies. G Ital Cardiol. 1999;29(6):607–615. [PubMed] [Google Scholar]
Posted in Uncategorized |
Cath lab nightmares may be a cliche word for all of us. Still, It has become a mandatory topic in any cardiology conferences and live workshops. These sessions are always popular and crowded as Interventional cardiologists are eager to get tips from other experts, on what to and what not to do in the cath lab in crisis situations. While stuck in an unexpected problem, these tips really help us come out of this, with shared expertise, presence of mind, skills, innovation, etc.
I asked them, what can be done about this ? “Nothing much” was the unanimous response
Final message
To end on a positive note, nothing is Impossible. Let us first start feeling this moral nightmare, and quell it at its origin. Fortunately, this doesn’t need sophisticated hardware. All we require is a little bit of righteous & peaceful application of mind in the way we learn and practice science.
Posted in Uncategorized |
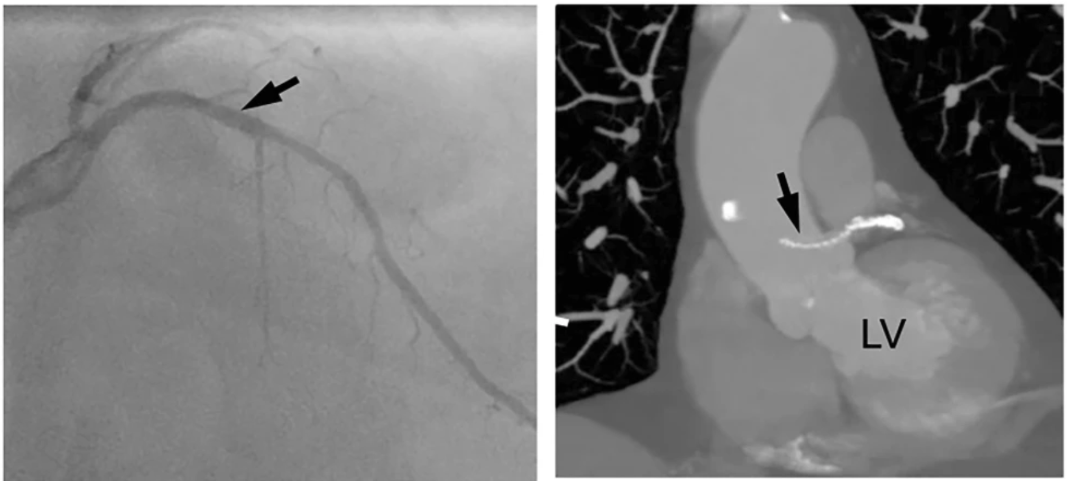
Pure science
Whenever possible ,before doing a coronary revascularisation procedure , check twice the segments you try to perfuse is really short of blood supply and truly needs the procedure. Don’t ever waste your resources and try to blood-feed the dead myocardium. It’ can never be awakened !
Pragmatic science
I was conversing with my colleague recently , who has grown into suave , Interventional cardiologist with a huge academic & societal repute .He owns a personal cathlab and planning to get one more.
I learnt a non-academic reality lesson from him .
When planning myocardial revasascularisation, apart from myocardial viablity status, there is one more viability issue which is done in the account books of finance mangers across big hospitals. Its Cath lab viablity. Trust me, he used exactly the same word ! He went on to explain in detail , how, every day there must be a minimum number of procedures to keep the machine alive. Which is under the eagle eyes of the guys who funded the state of the art lab !
“So, what do you say,I asked him ?”
He was frank enough to admit, he felt always happy when he is able to convert angiograms into angioplasties.He went on to add , the Ideal CAG-PCI conversion ration should be atleast 3:1 or more.
“Whenver I hear such genuine statments from real world people , it pains, as it tends to confirm my assumptions ”
Final message
I am wondering with all my lost wisdom. Why should any cardiologist after 30 years of training, fight for cath lab viablity , and get into a conflict with the very organ they are supposed to care and protect.
When did we become so Inferior beings & fight for the survival of these life less machines ?
Meanwhile, major text books , has un-intentionally facilitated this academic deciet .They have largely taken away the sting out of the snake . Myocardial viablity , hibernating, stunned myocardium , are rarely given importance nowadays and made it appear taboo concepts,in cardiology academia.
Postamble.
Will be extremely happy if what is portrayed in this post is not really true.
Reference
Nandan S. Anavekar, Panithaya Chareonthaitawee, Jagat Narula, Bernard J. Gersh, Revascularization in Patients With Severe Left Ventricular Dysfunction: Is the Assessment of Viability Still Viable?,
Journal of the American College of Cardiology, Volume 67, Issue 24, 2016,Pages 2874-2887,
Posted in bio ethics, cardiology wisdom, cardiology-ethics, Cardiology-Statistics, cath lab tips and tricks, Medical education, Medical ethics, medical quotes, medical satistics, Two line sermons in cardiology, wisdom in cardiology | Tagged cath lab viablity vs myocardial viablity, myocardial viablity before pci ptca, myocardial viablity study | Leave a Comment »