Coronary artery lumen has unique character . Its well-known LAD diameter is not constant , it tapers in its distal course.(Unlike RCA which is more tubular ) It is estimated LAD looses 15 % of its diameter for every 30mm length.Fortunately LCX has no such long course to make tapering a visible threat. (Though it may still be an Issue !)
Is there a hemodyanmic purpose for this tapering in LAD ?
Should be, God never designs anatomy without a physiological purpose.We have to find it out.(Can it be meant for flow acceleration as the flow is entriely diastolic in LAD while in RCA its both in systole and diastole ?_
What is the relationship between tapering angle and final distal diameter?
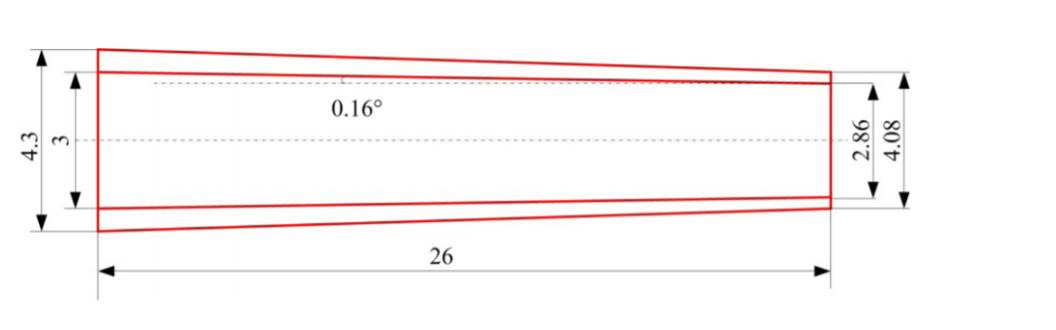
Schematic of an artery with a tapered angle of 0:16 .Ref XIANG SHEN Journal of Mechanics in Medicine and Biology Vol. 16, No. 8 (2016)
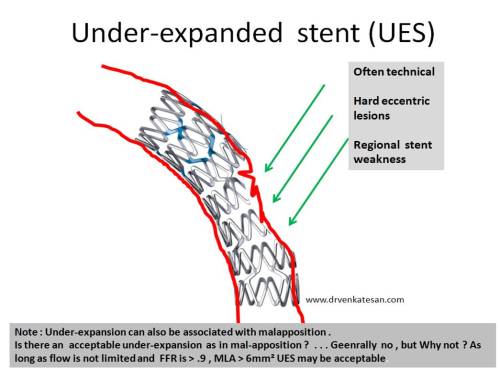
So, if you have a long lesion in proximal LAD and planning to stent with a 40 mm or long stent the distal end is hyperinflated by atleast 1.5mm, if we use a non tapered stent. Though , gain of extra diameter in distal segments might appear attractive, this may not work to our advantage , since it defies and distorts the natural hemodynamic flow pattern. Further , when you have tapering vessel, proximal optimisation becomes more important.
How about a tapering coronary stent ?
It should be a welcome addition to our already overflowing coronary hardware in fixing long lesions . Its still a surprise why only very few are making this type of stent.
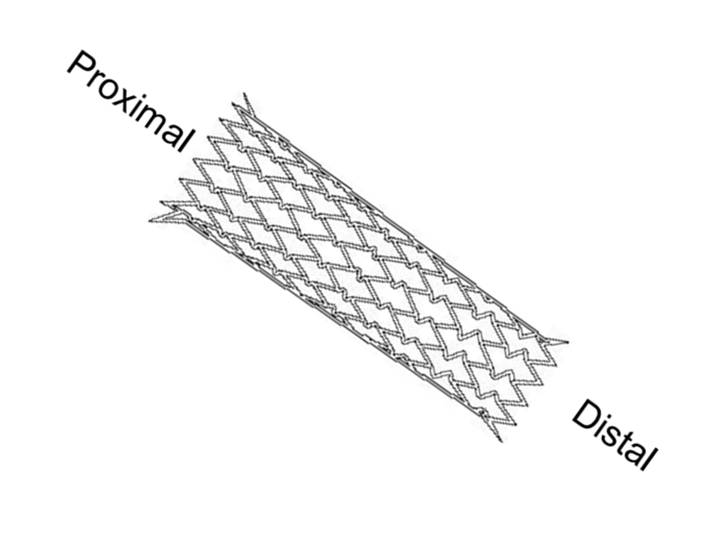
Meril has developed a tapered stent up to 60 mm long (Biomime morph).It should be useful in specific lesions sub types.Its worthwhile to note tapering stents are used more often in carotid artery .
Advantages of long tapering stent over two stents of different sizes.
- It avoid the vulnerable overlapping zone with double metallic load.
- Possibly cause less restenosis
- Low risk for stent fracture
- It reduces procedure time and of course the cost of stent by 50 %

Why the concept of Tapered stent is not that popular ?
I can only guess, probably lack of free availability and to a certian extent ignorance as well ! However ,current status about tapering stents is expected to evolve, though many cardiologist still feel it’s not clinicaly important issue to use a tubular stent in tapering vessel.
Alternative interventions in tapered vessel.
- Wall stent and other self expendable stents
- Tapered balloon Angioplasty (Laird Am Journal of card 1996)
Experts in this modality are welcome to share their experience.
Reference







{kind=link}