Dengue is a global infectious disease caused by Flavivirus (RNA) transmitted by day biting mosquitoes Ades aegypti .It is primarily a tropical or sub tropical disease , India is marked among the epicentre . 75% of dengue infections are asymptomatic. Among the remaining 25 % only 5 % develop severe dengue and a fraction of them go for a dreaded circulatory and bleeding complication leading to a likely fatality.Severe hypotension is the hall-mark in dengue shock .
The mechanism of shock
The sine-qua non of dengue shock is the capillary leak syndrome .This is due to some unknown vascular toxins acting in micro circulatory network making it exude fluid .This is something similar to septic shock where mal-distriubution of fluids in the extravascular or third spaces occur . This is also referred to as re-distributive or vasodilatory shock due to lack of effective circulatory volume. Significant serous cavity effusions (Both pleural effusion and ascites ) contribute to the shock syndrome . Meanwhile there can be accompanying fluid loss due to vomiting as well .Adding further complexity ,direct cardiac involvement in few in the form of myocarditis can cause lung congestion and confusing the true mechanism of shock .This has important hemodynamic implication as overzealous fluid therapy without recognising a possible myocarditis can be counter productive.Few sick patients will drag the lung into the vicious cycle ending up with ARDS , refractory hypoxia and worsening shock.
*To reemphasize , even though there are multiple components for dengue shock , the capillary leak is the dominant theme .
Timing of shock
The onset of shock peaks after 24-48 hours of fever .It may even be delayed well after subsidence of fever (Deffervescence phase )
Differential effect on diastolic and systole pressure
Dengue primarily drops the systolic pressure due to hypovolemia .The diastolic BP may be kept artificially high due the heightened adrenergic tone .This is ironical , as even the fluid is sequestrated into dead space patient may appear stable but it can fall dramatically without any warning once the sympathetic reserve is exhausted .This is the hallmark of dengue circulatory shock .
*Note : Dengue shock typically narrows the pulse pressure, that’s responsible for the feeble thready pulse.This is in contrast to septic shock* where the PVR is low, pulse pressure is either normal or even apparently high.(* Not all situations)
Clue from hematocit regarding the status of shock
Initially the heamtocrit tends to increase (hemo-concentration ) as fluid extravasates . Later it strikes a balance as we attempt to replenish with fluids. During recovery as fluids reenter vascular compartment or due to sustained fluid therapy the hemo-dilution can occur and heamtocrit may fall.
How common is myocarditis in dengue fever ?
Fortunately ,dengue fever rarely affects the heart directly .(Of course, shock can be a killer even without involving the heart) Myocardits due to dengue virus is randomly reported in literature (Ref 3,4). My guess is , the true incidence should be far higher as most of the dengue cases are from countries where publications are rare ! Bed side echo will reveal a minimally dilated Left ventricle with global hypokinesia and moderate to severe LV dysfunction. No need to prove myocarditis by virology ,biopsy etc. ( (New onset LV dysfunction with S3 , tachycardia is suffice) .Treatment is only supportive and Inotropic agents may be helpful. Recovery in LV function is usually complete in those who survive.
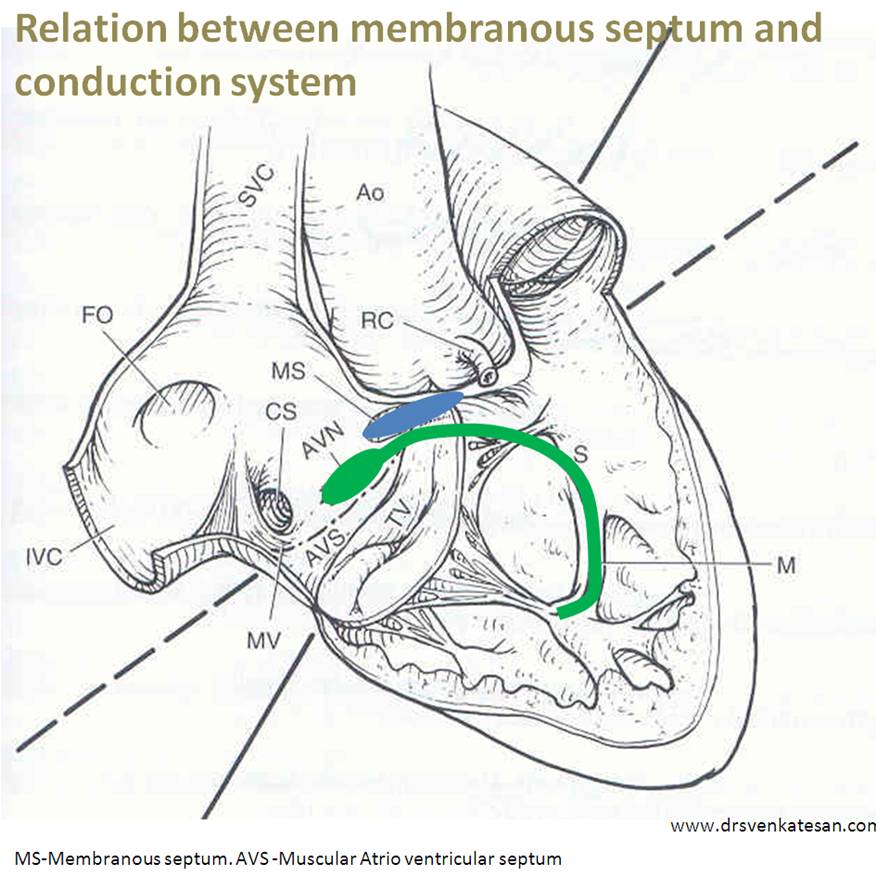
Acute pulmonary edema though expected with LV dysfunction , overzealous fluid therapy can be a trigger for this complication . Involvement of conduction system is another evidence for myocardial pathology. AV block (J Clin Diagn Res. 2015 May; 9(5) and Atrial fibrillation have been described in association with dengue.
Treatment
- Anticipation and prevention of onset of shock syndrome is the key .
- Careful monitoring of child is required.
- Altered mentation is vital clue
- Continuous fluid resuscitation is the only proven treatment .
- Platelet infusion is required in clinical bleeding generally <10000)
Steroids, Immuno-suppression ,globulin have limited or no value even in fulminant dengue fever .
Post-ample : Role of cardiologist in dengue shock .
Once , recently I was called to see a child with refractory dengue shock .It turned out to be a helpless consult for the parents who had great faith in me .They believed as a modern day cardiologist ( circulatory specialist ?) with sophisticated devices I will be able revive the vascular system .I regretted ,there is nothing specific can be done ,the entire circulatory system is leaking and had lost its tone ,we have to wait ,watch and pray .
I realised on that day , how these tiny mosquitoes can expose us . . . the much hyped cardio vascular specialist’s skills who live a celebrity life,hopping between cath labs , still unable to deliver at a critical time of need !
Reference :
1.Capillary leak syndrome in dengue fever.New Delhi: WHO Regional Office for South-East Asia and Manila: WHO Regional Office for the Western Pacific.Dec-2011
2.

3.Kabra SK, Juneja R, Madhulika, Myocardiald ysfunction in children with dengue haemorrhagic fever.Natl Med J India.1998Mar-Apr; 11(2): 59-61
4.Wali JP, Biswas A, Chandra S, Cardiac involvement in Dengue Haemorrhagic Fever.Int J Cardiol.1998 Mar 13; 64(1): 31-6.
5.Horta Veloso H, Ferreira Júnior JA, . Acute atrial fibrillation during dengue hemorrhagic fever.Braz J Infect Dis.2003 Dec; 7(6): 418-22
 Timing of diastolic MR
Timing of diastolic MR