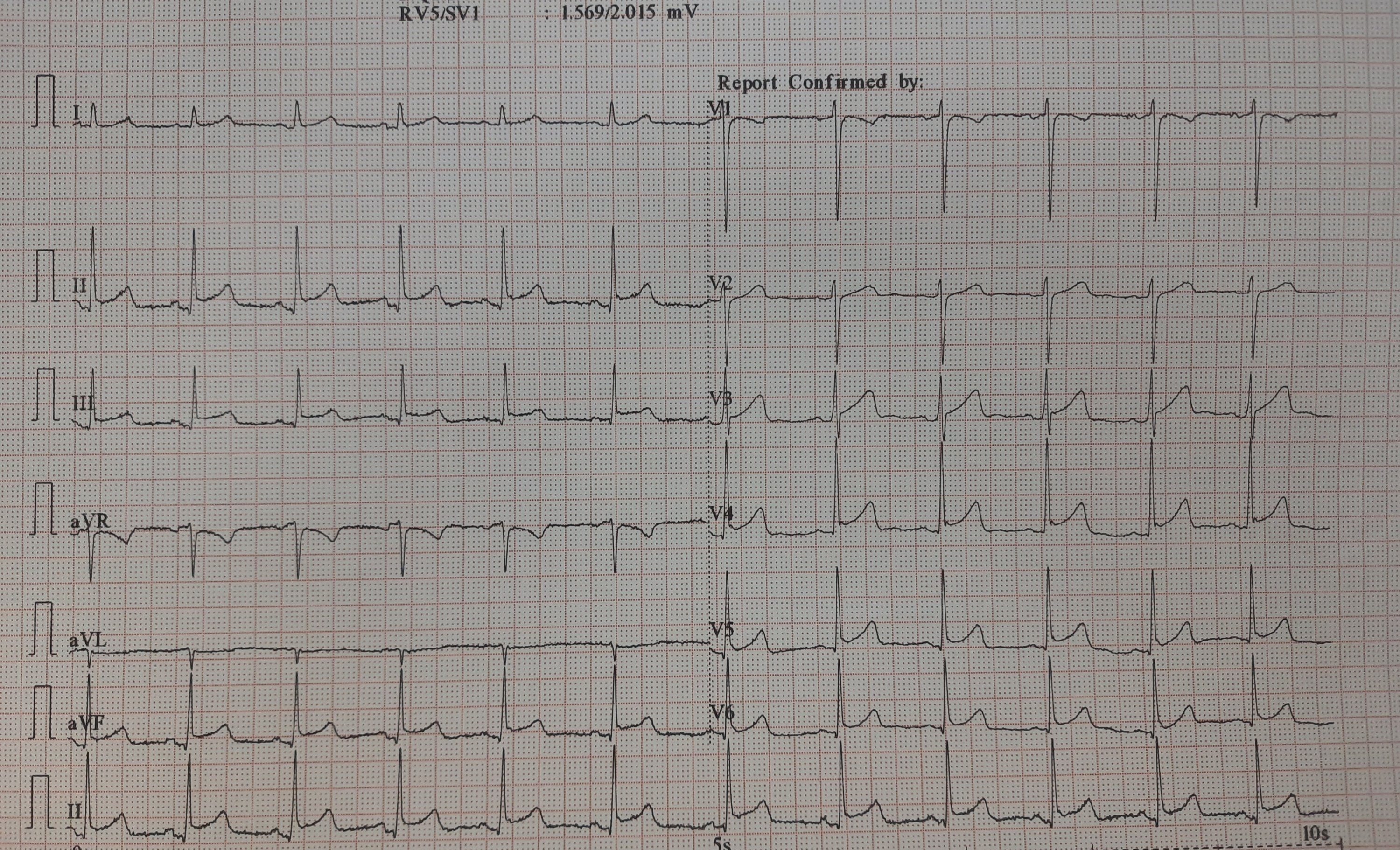
This is an ECG of a 25-year-old, recorded in master health check-up.
It would be mind-boggling to know the prevalence of such ERS patterns in the general population. One estimate suggests it could be anywhere between 3 to 13 % depending upon the criteria used. Let us assume the mean as 5 %. Then, it would be 30 crores of human beings in our habitat show this ECG pattern. If applied, in my city Chennai alone 5 lakh people could carry this tag.
While it is true, some forms of ERS and J wave syndrome can be markers of serious ventricular arrhythmias, either spontaneous or at times of Ischemia. Currently, It has become a fad, in cardiology academic circles*, to propagate the idea that ERS is no longer a benign condition. This is not acceptable at any degree of cognition. This happened mainly after few studies in powerful journals created some alarmist views. (*Maybe there is a bit of truth there. I still have doubts about whether we interpreted the Michel Haïssaguerre study properly)
Final message
ERS is a widely prevalent normal ECG variation with a minuscule risk. High-risk subsets need to be screened only if the J waves encroach and spill dangerously into the ST segment as well. Of course, this pattern is of serious concern if there is a family history of young SCDs has occurred.
Reference
Here is a good review of this topic by





