Heart is not like a rigid structure built with bricks . . . . so , its too architectural mindset to describe cardiac chambers to be made up of walls. Rather , Its a four chambered muscle mass moulded together in a complex 3D interface with distinct surfaces rather than walls. It’s also important to realise, since the heart is positioned (rather hanging )delicately in the middle mediastinum resting on the diaphragm , its subjected to one more dynamism due to respiratory motion blurring the definition of surfaces as well. (Vertical vs Horizontal)

Posterior surface is now referred to as infero-posterior
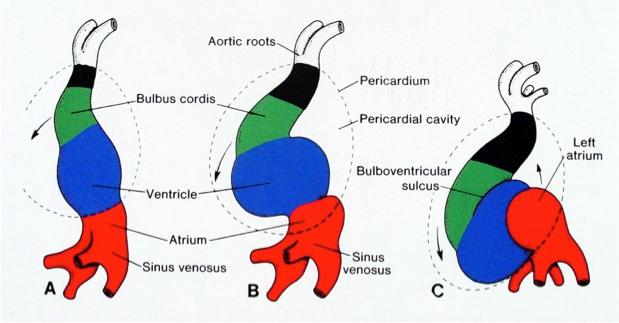
The posterior aspect of heart contains essentially the venous channels and the atrium (LA in particular)pulmonary veins and coronary sinus. This happens right from 8 week heart open stage when venous end of lower straight heart tube folds up and posteriorly .
It should be recalled only a small portion of lower aspect of posterior wall is alloted to left ventrilce.Instead the Infero diaphragmatic surface is formed by two-thirds the LV and one-third Right ventricle.

Image courtesy : From the great Netter
Nomenclature issue
The term posterior wall is now abandoned in most Echocardiography texts its replaced by inferior .The implication is more for Electrophysiologists with reference to accessory pathway localization
What is true posterior wall MI ?
As discussed before ,posterior surface of heart is different from posterior aspect of left and and right ventricle.
What does leads V7 V8 V9 record ?
It actually records electrical signals arising from posterior aspect of heart. Left atrium, pulmonary vein along with insulatory effect of lungs dampens the potential . This makes the sensitivity of ST elevation in posterior MI is low.
Blood supply of posterior surface
It’s highly variable.Both RCA and LCX arteries contribute with its posterior left ventricular branches (PLV)
It can be inferred , LCX has more territorial rights than RCA in this unique zone of heart as the artery covers more posterior areas.
Read a related article
Back pain from anterior MI : Is it possible ?





