World heart day is being celebrated every year on September 29th ,Initiated by the World heart federation with a genuine purpose, vision & goal. It has become big hit in recent times. In India, the theme has captured the imagination of the main stream media . Every one wants to propogate a message. I am not an exception. Please bear with this skewed message “One for the patients and the other for the self” !
Interventional cardiologists generally do not believe (rather relish) in simple balloon dilatations to remove any vascular blocks. It is a mundane job for their talent-rich hands. After conquering the coronaries, we made exclusive valvular stents. No surprise, TAVR has taken over the aortic interventions with all its glamour and vigor, though it is definitely not an ideal choice in all.
SCAI, the prestigious journal in Interventional cardiology has a recent article , that has a not-so pleasant message for TAVR lovers.
It seems reasonable to believe BAV, with considerable improvement in hardware, technology, and expertise can be an alternative to TAVR in high-risk aortic stenosis in a substantial number of patients.
It is also worth pondering over a less discussed aspect of BAV. The apparent high adverse events with BAV in calcific AS reported in the past-PARTNER days are now proven to be either exaggerated, outdated, or outright false. (For the evidence seekers, there was never a control BAV arm in none of those big studies on TAVR. It was purely a Surgery vs TAVR study. (A flaw in the aim of the study?) They may call it unethical to have a BAV limb, my understanding is, the absence of which is more unethical, as we claim superiority of TAVR without a less invasive option of BAV as control )
The fact of the matter is, in many centers, the risk of sudden death or acute aortic regurgitation is either comparable to or acceptable when compared to transcatheter aortic valve replacement (TAVR). It is worth emphasizing that BAV can be performed regardless of the load and location of calcium, while TAVR requires minimum elastic calcific load assistance to hold the valve in place. Further, BAV-related issues can now be effectively managed with efficient hemodynamic management.
Final message
If not scientiifally discriminated*, new age BAV can upgrade itself from the “self imposed contraindication” to, a sustainable alternative to TAVR ,atleast in selected sub-group of patients with isolated AS. This reality sould be perceived not only in the cost perspective, but also in the overall superiority in avoiding all those menacing complications with TAVR.
Postamble
*Very difficult task for the humble balloon to prevail over glamarous TAVR. Still,there is some hope(.We can get it from the emerging DEB story, where balloons are able to get rid of stents from the coronaries).
Reference
This is an interesting and important paper in the BAV vs TAVR debate. The funny thing is, even after reading it twice, I am unable to clarify which procedure this paper really favors!
This quote is being sent for the annual meet of “Right care movement” I know ,this can sound outrageous, permissble limits of abuse ? Up to 2% or 5% ? Let it be anything . Meanwhile try to enlighten yourself , the key differences between misuse & abuse.
Discussing lifestyle modification is an essential cliché in every preventive cardiology consult, For most, it still means good nutrition exercise, and stress relief. It is true, that the average human longevity has increased considerably in the last century. However, this apparent gain in life expectancy by the stunning discoveries in science ( 10 years ?) has already been eaten up, by the self-inflicted, poor styles in life. The new kid on the block, i.e. social media is playing a powerful amplifying effect.
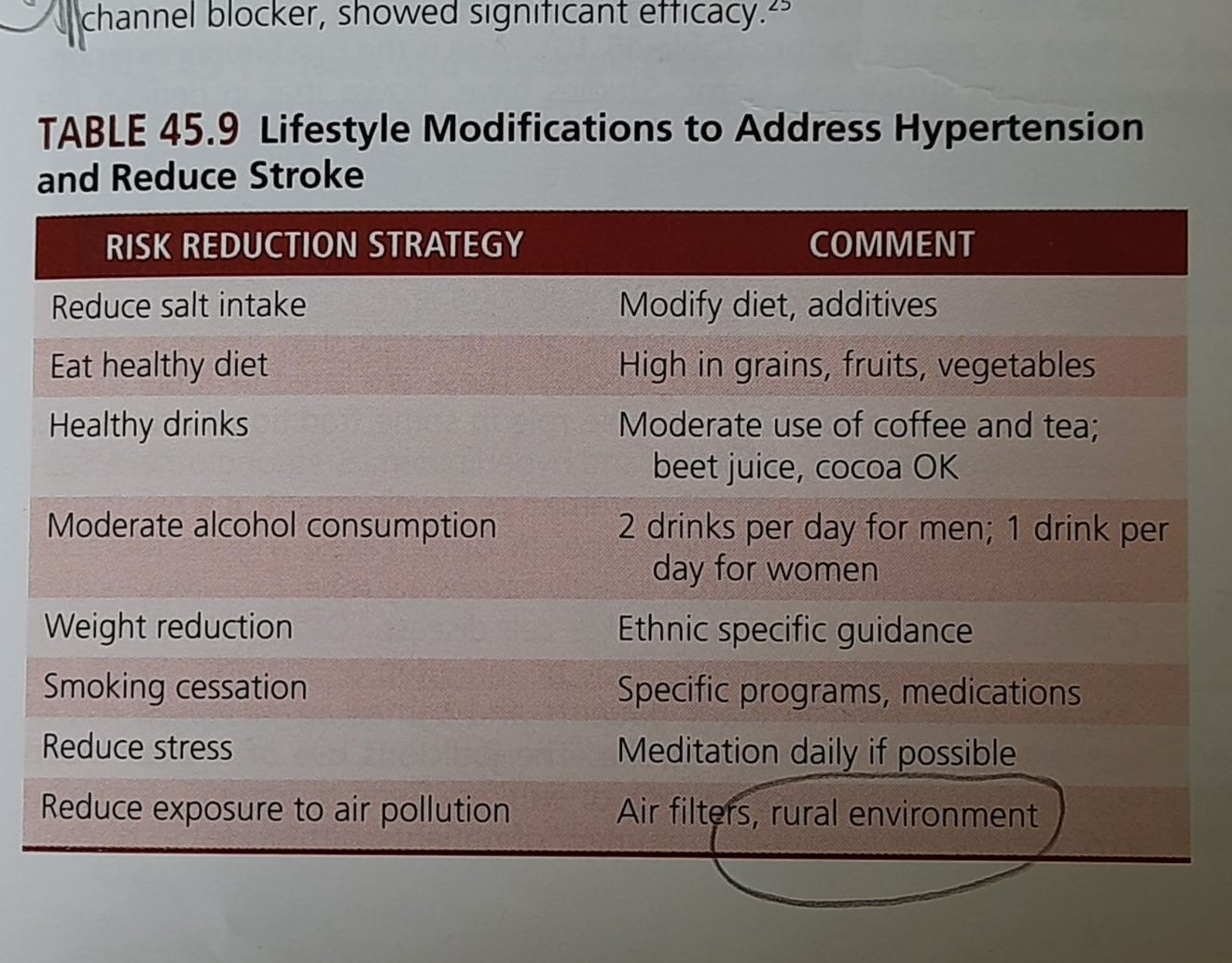
Spot a new entry in lifestyle interventions.
Here is a fresh list of lifestyle modifications from the latest edition textbook of heart disease by Dr.Braunwald, considered the bible of Cardiology. Not at all surprised, to note the new entrant at the bottom of the list.
Yes, It is asking us to consider moving out, from the lovely city life to the countryside, and gift a pure and peaceful life to our vascular endothelium, which is devoid of PM2.5, NO2, Carbon monoxide (CO) Sulphur dioxide (SO2), etc.
Final message
I would expect the World Health Organization (WHO) to declare ” unregulated urbanization” as a communicable disease and include it in the ICD code sooner or later. (Air pollution is a masquerading term though!) .The urgency is real, since the apparent gain in life, due to modern medical therapeutics is getting rapidly eroded.
No more evidence is required to emphasize the fact, that enforced rural living is going to be an important CVD Intervention for the future. If someone (or any organization ) is still doing research to confirm this, please realize you are wasting time, stop it, and get on with corrective action along with the WHO’s other SDG goals.
Is it a STEMI or Non -STEMI ? The apparently realistic, but dichotomous thinking about ACS among physicians is existing for quite a long time. However, since the underlying pathobiology being same , it is worth wondering whether the conventional bifurcation of ACS is fool -proof , when applied to management decisions. The rapidity and totality of plaque fissure, rupture ,eruption,or erosion and the subsequent response of the local hemorheological system, determine the ferocity of the event.
How to recognise all these deep intracellular events in bed side ? Unfortunately, still with a lot of gratitude, we have to rely on the humble ECG for early segregation of ACS ,initiation of treatment. (Truthfully, Waller, Einthoven and Lewis should still be celebrated as forefathers of ACS )
Though STEMI/NSTEMI show different faces of ACS, however, it makes little logic to have two big set of guidelines when a patient presents with ER with resting angina with variable ST/T changes* .(In the very early hours of ACS, ie just moments after biological trigger who can predict which patient will enter what path and evolve into STEMI or NSTEMI)
* Typically, predicting the ECG-plaque interplay in Wellens’s syndrome ,De-winter or for that matter , in any biphasic precardial T wave sydromes can stretch our coronary acumen to its limits.
Now, ESC 2023 task force hasrealised this .To bring bettter judgment with a open mind ,decided to merge STEMI/NSTEMI into a single guideline , of-couse a with different treatment flow paths for these two entites.
I could take three key messages from this new guidelines.
1.STEMI guidelines are largely unchanged. There is still a major role for fibrinolysis, if you realistically think, and decide, you can’t reperfuse in the cath lab within 120 minutes after arrival.(120 mts time clock should start, much earlier is different debate!)
2.In NSTEMI, there has been important downgrading in the urgency of intervention even in the high risk category (Early invasive <24 hrs from class 1 to 2A)
3. Aspirin and regular unfractioned Heparin continue to rule the ACS world in most situations across the entire spectrum of ACS, except during the short peri-procedural period ,we need the assistance of new powerful P2Y12 blockers like Prasugrel or Ticagrelol.
Prof. Robert Byrne, from Ireland, succinctly explains the new ACS guidelines
Final message
Knowledge must be allowed to evolve, without any conditions or denials. Backtracking is an essential expertise, which can be as important as looking forward.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.