
Original article
Chevalier B, Glatt B, Royer T, Guyon P. Placement of coronary stents in bifur-
cation lesions by the ‘culotte’ technique.Am J Cardiol 1998;82:943 – 949
Posted in cath lab tips and tricks, tagged cullotte technique for bifurcation, ptca pci tips on June 28, 2013| Leave a Comment »
Posted in Cardiology -Interventional -PCI, cath lab tips and tricks, tagged cath lab tips and tricks, ira vs nonira angioplasty, multivessel angioplasty in stemi, primary pci on May 19, 2013| Leave a Comment »
Multivessel PCI during acute STEMI is forbidden except in cardiogenic shock . (or in some very unstable patients without cardiogenic shock)
The reason
Still . . . in real world it is extremely difficult to curtail the urge to stent all eligible lesion during primary PCI !
How to avoid it ?
If the patient is poor or the insurance limit is low , the issue of multi vessel stenting does not arise at all !
Always ignore complex non IRA lesions during primary PCI. Be happy if a non IRA has a bifurcation lesion !
Still , some lovely looking lesions in non IRA would be tempting and inviting . Indulge at your own risk !
* Please remember if the proximal LAD has a non IRA lesion , it may be sensible to attempt simultaneous revascularisation even if the patient is stable !
Other unrealistic advice
Reference


Posted in cath lab tips and tricks, Hardware techniques tips, tagged preformed judkins right left, rca catheter, sones voda multipurpose judkins tiger on April 30, 2013| Leave a Comment »
Interventional cardiology has grown leaps and bound in the last few decades .We are able to clip the wings of mitral valve without surgery when it prolapses
We can deliver a huge aortic valve and fix it with wires .
But . . . we have no proper preformed guiding catheter that can sit into RCA ostium directly and snugly for a long time to enable complex RCA angioplasties !
An now try this one .
Here is a pending patent for a preformed RCA catheter
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology- coronary care, cath lab tips and tricks, tagged bifurcation lesion, bifurcation pci, carina plaque shift bifurcation lesion, medina classification, true bifurcation angle on April 7, 2013| Leave a Comment »
Posted in Cardiology -Interventional -PCI, Cardiology-Coronary artery disese, cath lab tips and tricks, cto chronic total occlusion, PCI PTCA Hardware, tagged chronic total occlusion, cto, tips and tricks on February 28, 2013| Leave a Comment »
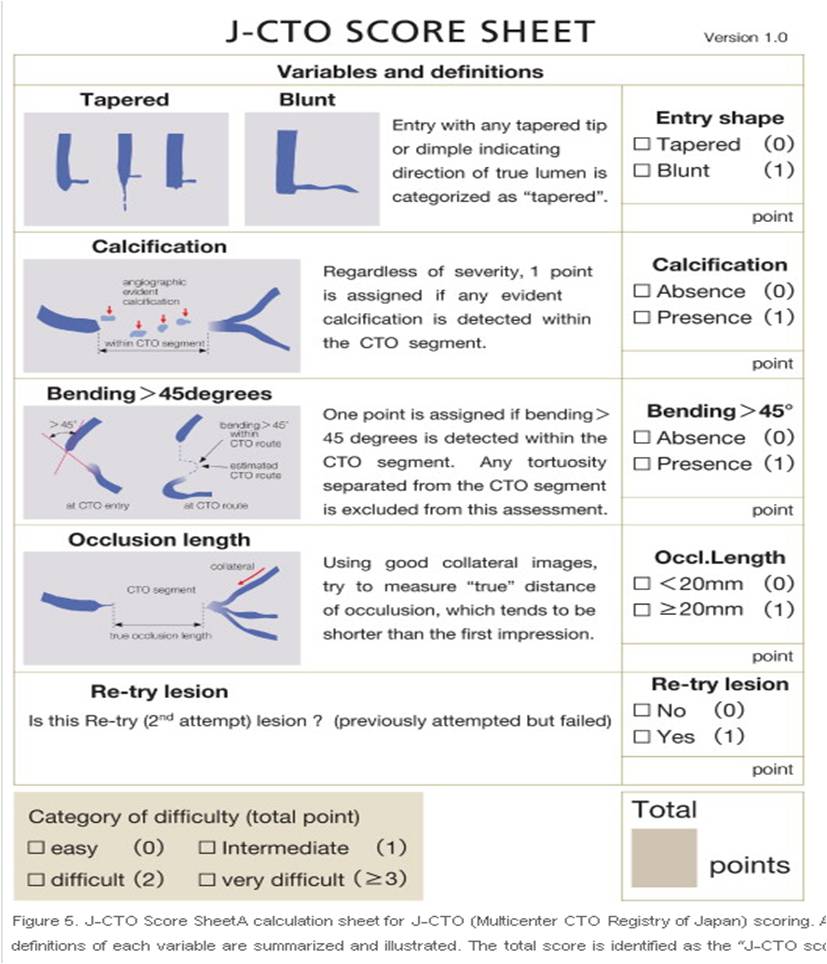
Japanese are the pioneers in CTO reopening .(I understand they do less CABG surgeries for religious reasons ) CTO is the ultimate test for cardiologist patience . it may take hours to open up a CTO (or even to abandon it .) Here is a success prediction tool from Japan .
Source courtesy : JACC: Cardiovascular Interventions Volume 4, Issue 2, February 2011
Reference
http://www.sciencedirect.com/science/article/pii/S193687981000912X
Posted in cardiology- coronary care, Cardiology-Coronary artery disese, cath lab tips and tricks, cto chronic total occlusion, Hardware techniques tips, tagged chronic total occlusion, cto, fielder xt, pci for cto, retrograde cto crossing, success in cto pci, tips and tricks on February 27, 2013| Leave a Comment »
Answer :
While each one of the above factor appears very much important morphology of the lesion is the clear winner ( Which includes , the content of the lesion , hardness , micro channels , thickness of the proximal and distal caps, the length and tortuosity of the CTO ( which is invisible ) the collateral status will ultimately determine the success)
It is becoming increasingly clear cardiologist expertise is getting less and less important .
Finally , it must be told to our younger generation of cardiologists , crossing a CTO and deploying a stent is not synonymous with success .It should result in long term sustained distal flow and make a significant impact on the patients symptoms (If at all any !) and survival.
Posted in Cardiology -Interventional -PCI, carotid interventions, cath lab tips and tricks, tagged catheter retrival of infective vegetation on September 30, 2012| 1 Comment »
Intra cardiac foreign bodies are frequent occurrences in clinical cardiology practice. The common ones are intra chamber clots , vegetations and rarely tumors. Some of these masses are very mobile are precariously attached to the cardiac strutures . It becomes a cardiac emergency as a major embolic event is imminent .
While surgery remains the mainstay approach in such situations , now it seems possible to trap these mobile masses with help of catheter and retrieval devices safely.
The only issue is , while retrieving these masses it should not be let into the circulation and result in embolisation . For this we can develop a porous net (Fishing net like ) that can be blown in the distal chamber or Aorta .

Devices can be structured in way that a single catheter can be used with different ports to capture and filter and retrieve the mass . ( vacuum enabled suction catheters can be additional option ) .The whole procedure can be accomplished with fluroscoy and fluroscopic guidance . Intra cardiac echocardiography might also contribute .
This innovation will be a great value addition to the interventional cardiology armamentarium ,would be be appreciated by clinical cardiologists . We in our tertiary teaching hospital have felt the need for a such a device quiet often .Currently many patients land up in surgical tables for the sole purpose of removing these clots and vegetations .Similarly left atrial clots becomes a contraindication for percutaneous mitral commissurotomy(PTMC) . Such capture devices can be very useful.
Posted in cath lab tips and tricks, Hardware techniques tips, tagged cath lab, cortical skills and cath lab, guidewire manipulation, guidewire torque feel, interventions in cto, tactile feel of guidewire, tips and tricks in cath lab on June 9, 2012| Leave a Comment »
Years ago , I remember asking my professor during a balloon mitral valvotomy workshop .
How is that , you are able to puncture the IAS effortlessly and efficiently sir ?
Every thing is in the feel Venkat , he used to say !
What feel ? I used to wonder !
Now , I realise the guide wires and catheters are just an extension of our hand and fingers.
When we tackle CTO lesions we should be able to feel and differentiate the capsule and dimple .
More sensitive hands (Brains) can tell whether the guide wire is poking the vessel wall or the lesion .
Of-course , now we have sophisticated OCT, IVUS, and camera tipped ( Is it really there ?) guide wires to guide us.
Still , a cardiologist who is able to feel the lesion intimately . . . would be a clear winner !
How to feel a lesion ? (Plaque palpation , Hitting the calcium , Feeling the thrombus ! Cuddling the foramen ovale etc )
Key word : Guide wire tactile sensitivity .We are familiar with guide wire torque .Now , a new technology that can transmit the feel of the target lesion , to the hands of the operator would be very much desirable .
Two point discrimination and temporal cortex plays a critical role here. Irrespective of the hard ware used , how the brain perceives touch is going to determine whether you are going to cross a difficult lesion .
Can you electronically amplify tactile feeling like sound amplification ?
It may be possible in near future. But it has other issues like hypersensitiveness
Can a physician with defective cortical sensory system face difficulty in catheter based interventions ?
I have observed at least two cardiologists with diabetes , acknowledging major difficulty to feel the palque and cross the lesion (Due to autonomic neuropathy ?) With many cardiologists rapidly aging , the quest for intervention goes unabated (Still unwilling to quit ! ) one may experience cortical dementia as a hurdle for guide wire manipulation . These issues need to be tested in real world .
Final message
It is fascinating , how the feel of coronary plaque reaches our brain . It is picked by the tip of guide wire , travels about 150cm , handing over the weak signals across the gloved fingers , reaching all the way through cervical spinal cord and spino-thalamic tracts , brainstem and finally to the cortex.
There are multitude of factors that determine the success of complex angioplasties . I realised suddenly , Intact cortical sense could be an important one, among them . Let us train our brain centres for this specific sensation of cath lab hardware . After all , the brain is maneuvering force in any cardaic intervention !




