Preamble * This article is meant specifically for cardiac professionals only .There has been so many queries to me about this device Megavac from patients and public. It is just another tool for assisting angioplasty in very special situations . Successful angioplasty can be performed without the need for such devices 9 out of 10 times. I request the non medical readers to skip this article and follow your cardiologist’s advice and don’t get unduly anxious.
Dr Venkatesan .Chennai.India
If thrombus is the chief culprit in any vascular emergency there can be no second thoughts as it needs immediate arrest without warrant! (STEMI,Acute pulmonary embolism , DVT, Acute limb ischemia etc) Since pharmacological lysis of thrombus is easy and be done immediately it will continue to play a major role still , in many clinical situations that critically compromise organ function .
However , large thrombus burden (or in which medical therapy fails to do a good job ) we must intervene mechanically to change the course of event.Though vascular surgery is a definitive option its always better we try out catheter based thrombectomy.
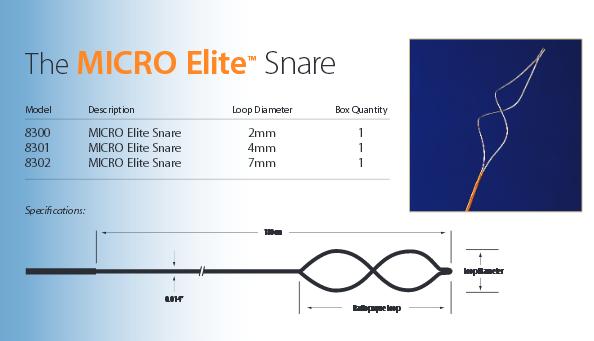
Many hardwares are being developed in the recent times. Aspiration catheters, baskets etc * .This one from vascular capture (Minnesota USA) appear promising as its a universal capture device that can be used anywhere coronary , pulmonary or even in deep veins .
Clinical case examples using megavac : Video
*Few examples of Thrombectomy devices.
1.They can be mechanical rotational devices like Amplatz Thrombectomy Device (ATD) Microvena, Straub Rotarex (Straub Medical, Wangs, Switzerland) and the Tretorotola Device ( Arrow International, USA) employ a high-velocity rotating helix or nitinol cage that macerates the thrombus.Disadvantage is endothelial contact with moving mechanical parts.
2.The Angiojet device (Angiojet; Possis, Minneapolis, USA) uses a rheolytic mechanism with possible less endothelial injury as there is no true contact with endothelium.
3.Ultrasound mediated lyis ( EKOS Endowave (EKOS Corporation, USA) and Omniwave (Omnisonics Medical Technologies, USA) fragment with high frequency ultrasonic waves.