Holter monitoring is the Initial test for all those with documented syncope (or Pre syncope ) with suspected cardiac arrhythmia .It is a 24 hour ambulatory ECG monitoring , expected to pick up any electrical abnormality and its correlation with the resultant symptom if any. Though the test looks attractive , the diagnostic yield is far less. (About 10%) .The reason being the episodes can be rare to be missed by 24hr sample time. We have extended Holter (48hr) , Event monitors , Loop recorders and implantable devices that can record ECG for extended periods.(18 Months ,Reveal Plus Medtronic) that improve the yield up to 45%.
One common issue that often confuse us while reporting Holter is, the pauses that occur during day / night .
What is the significance of these pauses * ? Nocturnal vs Daytime
Pauses are obviously significant when the patient is awake . It is generally accepted pauses more than 3 seconds during day time (ie Heart rate of < 20/mt ) is significant . This is logical , as pauses more than that, is expected to cause syncope ( or atleast pre-syncope ).The problem comes when you document pauses more than 3 seconds without any symptoms . Then this difficult question comes up ,At what degree of pause syncope occurs ? How is that some persons mange even prolonged pauses with just giddiness.(Good overall vascular integrity and tone ! )
We know such pauses are especially common during sleep. How does the brain react when pauses occur during sleep ? as there is no question of fall as such and loss of muscle tone is non existing.
*Please note ,when we say pause we mean only Sinus pause , Pauses due to AV blocks are very significant
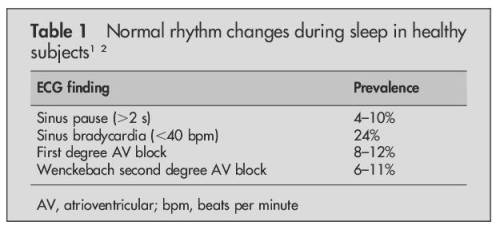
Source : Brodsky M, Wu D, Denes P,et al.Am J Cardiol 1977; .
Dramatic pauses during sleep do occur
There has been prolonged pauses reported during sleep without fatality . A 35 second nocturnal pause resulting in seizures has been documented by implantable recorders.(Mairesse 2003)
Causes for prolonged pauses
- Sinus node dysfunction
- Obstructive sleep apnea
- High dose beta blockers therapy
Final message
Most bradycardic episodes during sleep are benign.This is due to depressed autonomic control during sleep. Holter interpretation is primarily done with awake rhythm data in most individuals .So, empirically shall we fix a 5 second pause as significant during sleep ? We don’t know.While this may seem applicable even with structural heart disease , one may be vigilant while interpreting the nocturnal pauses in this population .
Caution
** Please note, all these rhythm monitoring extravaganza is meant for people with equivocal symptoms .Patients with well documented syncope with ECG features suggestive of cardiac rhythm disorders would never require these tests and go for pacemaker straightaway.
Reference
4.Arrhythmias documented by 24 hour continuous electrocardiographic monitoring in 50 male medical students without apparent heart disease. Brodsky M, Wu D, Denes P,et al.Am J Cardiol 1977;39:390–5.
For Advanced readers
Read Full Post »







{kind=link}