“In one sense, meta-analysis would come closer to a milder form of ethical plagiarism”
Can meta-analysis really be called as original scientific research ?
No it is not, but some may say yes. It is very difficult to dispute either. But, the fact of the matter is, meta-analyses are not a true science of innovation. It is using some others’ work( sort of intellectual steal ?) done by a group of scientists interested in the same research topic, trying to squeeze more info from these studies. It is a glorified group journal club activity.
Image source & Courtesy http://www.inquasar.com
At best, meta-analysis can be referred to as knowledge and evidence aggregation. Surprisingly, mostof the academia seems to give more weight to meta-analysis, disproportionately more than the original researchers. This is because meta-analytic scientists backed by big journals claim, they can bring out more info out of the original. The assumed scientific superiority of meta-analysis is expected to be downgraded soon, as these sort of evidence aggregation can be done easily by any AI-powered engines. Network meta analysis, by dedicated medical scholastic AI networks can do this in a fraction of a second.
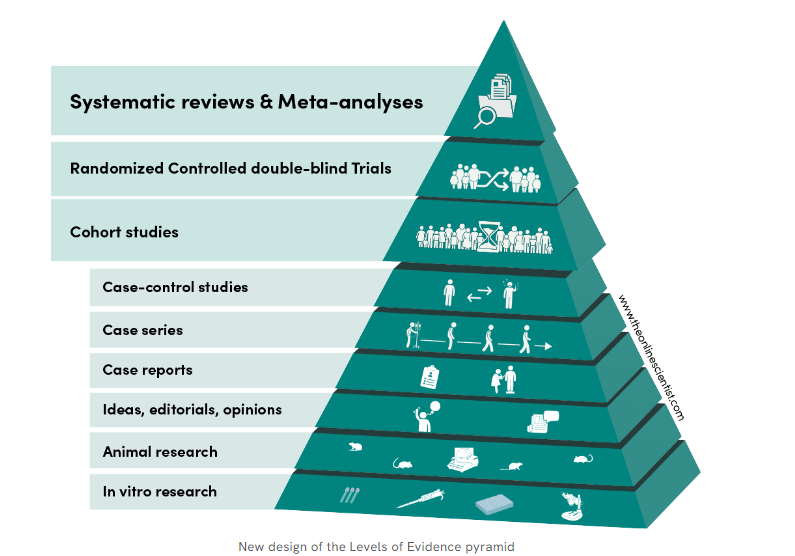
Meta analyses as of now is sitting proudly as crowning glory at the top of evidence pyramid. This is one of the reasons for the false glory surrounding anyone (or anything ) associated with meta-analyses. I doubt whether it really deserve the top slot. (An excellent debate between RCT vs metanalysis) Wish, the meta-analysis taste its own medicine at least once. We need to have a meta-analysis to show it is really superior to other forms of evidence. I cant find one as yet.
What about systematic review ? This looks better, as it has less statistical content , and the researcher is at least compelled to go deep and get enlightened on the topic as they spend months together on the topic.
How is meta analysis different from original research?
There is no new data collection ,no primary hypothesis testing . It primarily focus on summarizing existing evidence. To do it properly, there are certain standards.
- PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)
- Cochrane Handbook for Systematic Reviews of Interventions
- MOOSE (Meta-analysis of Observational Studies in Epidemiology)
Positive side of metanalysis
While meta-analyses aren’t original research, it’s a crucial tool for evidence synthesis, research translation informed decision-making.
Flaws of metanalysis
It is a academic business with done studies. So it is 100% retrospective. It might come with irreversible errors. Unless every error in the past studies is accounted for and curated the result of meta-analysis, it can never be foolproof.
Should we get permission from all the authors who did their original studies before doing a meta-analysis?
As long as fair use criteria applies there is no need , but a moral obligation is definitely there . Other wise metanalyses will come closer to a milder form of academic plagiarism of others’ work. (Of course legally and scientifically approved)
Final message
In the world of true scientific research, meta-analyses can not be considered as great scientific work. It is just evidence aggregation, which of course could be meaningful if and only if the studies taken were done properly.
However, meta-analysis has undisputed value in aggregating rare cases, scenarios, diseases, and problems where there are very few published studies. Collecting them together in an organized fashion serves a real good purpose.
Reference
1.Pearson K. Report on certain enteric fever inoculation statistics. Br Med J. 1904;3:1243–6.















{kind=link}