
Posted in Quotes, Uncategorized, wisdom in cardiology | Tagged best quotes in medical ethics, dr s venkatesan, dr venkat quotes, madars medical college, medical education, medical ethics, venkatesan sanagreddi |
We have enough evidence to question the superiority of the presumably best practice in cardiac pacing namely dual chamber pacing. Apparently, the DDD failed to show gross benefits in both AV block as well as sinus node dysfunction. (UKPACE, MODE-Selection Trial) in studies done nearly two decades ago.
It is 2022. Here is one more study in the Indian heart journal, coming up from JIPMER Pondycherry,on this concept. It is an intelligently designed cross-over study. The same patients were switched between DDD and VVI modes. This study reaffirmed the lack of appreciable hemodynamic and clinical benefits with DDD mode yet again.
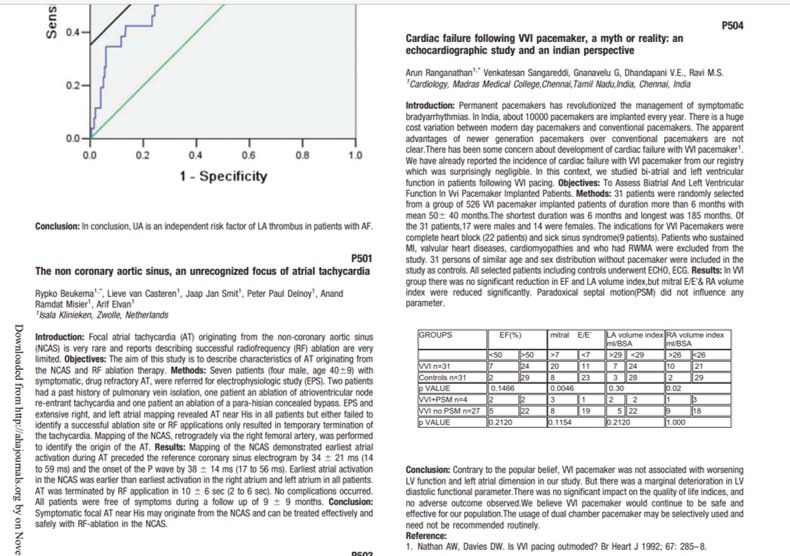
We have also contributed a little on this issue. It was found cardiac failure in VVI pacing was not a real big issue in the long-term follow-up. We presented and published in world congrees of cardiology Dubai 2012, and Circulation journal.
How is that? A dual chamber pacer with AV synchrony fails to show a hemodynamic benefit?
The answer is simple..VV desynchrony is a common denominator for both VVI and DDD pacers. Providing AV synchrony without VV synchrony doesn’t make real sense in the long term to overcome the altered physiology, Still, DDD pacing continues to enjoy a popular mandate by hiding behind a vague outcome measure called quality of life.
What is the physiological pacing then?
Just because, DDD and VVI pacers are equipoise, can we presume the new pacing kid LBBB pacing would be physiological? We wish so, but unless and until we replicate the entire conducting system right from SA, and the AV node which includes many miles length of delicate Purkinje cables, every pacing system we use is currently pathological. (If that sounds too harsh, let’s make it non-physiological)
Having said that, VVI pacing is one of the most remarkable Inventions in medical science since the last century, that plays God’s own function and gives a new lease of life to all those patients with critical AV blocks and trouble some SNDs.
Final message
It may be difficult to digest for true scientists. Restoring the atrial booster pump is not bringing in the desired benefits. It is clear that VVI pacing will never become obsolete. This fact was established long before. We must argue and wonder, why we need to keep proving a scientific truth again and again? There could be a good justification too. Real-time cardiologist behavioral patterns clearly tell us, as a genre, they often struggle to get detached from futile modalities even after good published evidence (PCI for CTO, Revascularisation for Ischemic DCM, are a few more examples)
Posted in Pace maker Tips and tricks, Uncategorized | Tagged pacemaker mode selection, vvi vs ddd pacing |
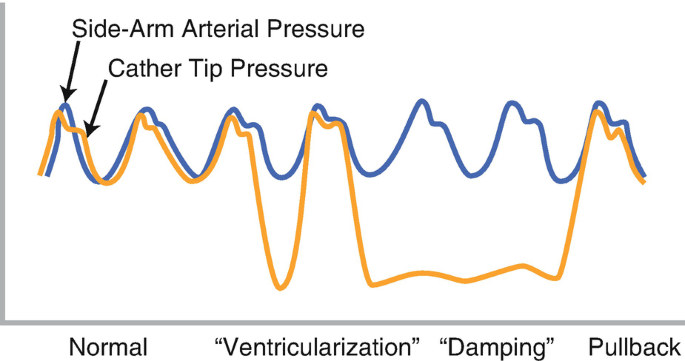
“Never take your eyes off the monitor and the pressure curve” It is one of the basic instructions given to the fellows & technicians as they start engaging the coronary artery and Intubating the coronary ostium in their early cath lab postings. There are two commonly heard noise bites in the cath lab for the beginner. 1. Damping 2.Ventricularization.
Damping
It is the deformation of the normal arterial pressure curve, with a blunting of both systolic and diastolic pressure that drops compared to aortic pressure. Extreme damping can mimic a straight line with few wavy undulations. It means the forward flow is impeded as the catheter might be blocking the coronary flow at least partially, if not completely. Immediate pull back and adjustment of catheter is required to prevent adverse events that includes cardiac arrest. (Of course, catheter kinks, blocks, and air in a circuit are to be ruled out first)
Mechanism of damping
- The catheter tip is too large for the ostium.(Technical)
- A left main or RCA ostial lesion*(Most significant clinically)
- The coronary artery wall is thin and goes for spasm
- Catheter diameter is too small and glides into the coronary artery (The catheter tip hitches against the lateral wall of the coronary artery often over a plaque, a silently staged perfect setting for a dissection )
Unique features in RCA damping
In RCA, damping could simply mean it has engaged conus branch. Damping is more common in RCA and it tends to get sucked in deeper for two reasons. We know , the RCA catheter is not preformed, the tip seeks the ostium, looking for a negative pulling pressure from within the RCA. Further, unlike the LCA, the flow in RCA is continuous in both systole and diastole. Another possible factor is the inspiratory swings of RV transmural pressure is more than LV.
Transient bradycardia due to compromise of SA /AV nodal flow is common. It is well known that RVOT is a thin and VPD-prone zone , compared toLVOT. Hence it is more vulnerable to ischemia and triggers a VT/VF if damping is prolonged in RCA.
Ventricularization

This is tracing during the engaging of a left main ostial stenosis. The diastolic pressure drops on the third complex, and the pulse pressure becomes large . Note the small “a ” wave slur as well near the diastolic nadir. The aortic pressure curve is restored once tip adjustment is done. Image courtesy Thoraci key.https://thoracickey.com/coronary-angiography-3/
It simply means the pressure curve starts looking like a ventricular pressure curve. The issue is not that simple. It is still a mystery, how could the coronary artery pick up ventricular pressure. In fact, it doesn’t. It was initially thought to be either deformed aortic pressure or a wedged coronary artery pressure .or a combination of the two.
It s now accepted it’s due to total occlusion of the coronary artery the ventricle muscle sucks the catheter and pulls the diastolic pressure markedly down even lower than LVEDP. The systolic pressure also falls but not much of it is noticed.The fact that ventriculaization happens less commonly with RCA gave us a clue to its mechanism. (Most of the RCA travels over RV and since RV muscle mass wields less negative suction force )
How to differentiate true LV location from ventricularization?
If the catheter enters the LV cavity, the systolic pressure will match that of aortic systolic pressure and diastole will reach the LVEDP. In ventricularization there can be a slight drop of the systolic pressure, but the diastolic is the one goes far down. Further, the ascending limb is shallower, the descending limb is steeper in coronary ventricularization. Apart from this if we carefully look “a” waves will be visible in ventricularisation in the late diastolic phase.(Could it be the modified Incisura ?)
Relationship between damping and ventricularization ?
Discussing damping and ventricularization together is more of an academic tradition. Please realize, both may not be two exclusive entities. In fact, they can occur at the same time, or sequentially or interchangeably if the catheter tip swings back to partial to total occlusion and vice versa. if complete wedging occurs it becomes ventriculariszation.
Which is more dangerous damping or ventricularization?
How can you ask such a question? Both can be harbingers of serious hemodynamic issues if ignored and accidentally injected, The dreaded one is the dissection. Apart from mechanical injury, Injecting dye during damping or ventricularization causes dye stasis, and may trigger VT or VF if it is prolonged. There is a biochemical component too. As the contrast swirls around for a few seconds it can cause transient hypocalcemia by chelating this cation.
I don’t have a clear answer to the above query. In my understanding, forceful injections during ventricularization could be more riskier as injection happens over a total occlusion in a wedged position and dye has direct access to the microcirculatory bed. It is true, expert cardiologists do shoot in damped positions occasionally to see the anatomy quickly. They may be your mentors, still don’t learn this trick, till you become a true expert (Famously referred to as hit and run technique)
How to overcome these pressure curve malformations?
Most times, it is a simple technical artifact issue. Deep Intubation with an oversized catheter could be the commonest cause in the otherwise normal coronary artery. Proper catheter sizing, angle of alignment, and adjustment is the key. If it is a spasm nitroglycerine might help. Using catheters with side-hole perfusion catheters is an option in difficult anatomies. Mind you, side holed guide is a two-edged weapon, it can mask true hemodynamic adversaries by falsely showing a good aortic pressure tracing.
(One of the good cath lab habits is to have a look around the patient face at least once in a while when performing complex procedures. We have many times recognized serious hemodynamic issues only after the patient starts behaving bizarrely due to hypotension. Pressure curves can fool you, but patience will never.)
Final message
Recognizing abnormal waveforms during engagement is a crucial step for the beginner (Experts can’t ignore though) Please remember LMCA stenosis should be the default alarm for any damped pressure curve as you engage the LCA. If you take things casually consequences can be lethal for the patient as well as the consultant in charge.(Fellows can’t take it lighter though). It is an undisclosed fact, that many of the serious complications in the cath lab happen not out of ignorance or lack of expertise, but because of ignoring some basic principles and lack of cath lab discipline.
Reference
1.Baim DS, ed. Grossman’s Cardiac Catheterization, Angiography, and Intervention. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006. 2. Judkins MP. Selective coronary arteriography, a percutaneous transfemoral technique. Radiology 1967;89:815.
2.T Pacold I, Hwang MH, Piao ZE, . The mechanism and significance of ventricularization of intracoronary pressure during coronary angiography.Am Heart J. 1989 Dec;118(6):1160-
Posted in Uncategorized | Tagged coronary artery damping and ventricularization, Damping and ventricularization, ventricularization |

Though all of us are aware, the incidence of heart failure is increasing exponentially and is the leading cause of global disease mortality, what we fail to understand is, we still lack a good definition cardiac failure.
Defining HF based on EF% is convenient but adds more complexity, and is less scientific too. Still, as of now, we have adopted this. I think, one of the important factors that apparently increased the incidence of HF is the creation of an entity called HFpEF. (Formerly diastolic heart failure)
Thanks to ESC, we have a consensus document, which has defined HFpEF based on functional, morphological, and biochemical features. This is a more refined model from the original Mayo clinic H2FpEF score.
Both are given below.


Can we diagnose clinically significant HFpEF, without pulmonary hypertension?
In my understanding, the answer is No.
Looking at the two schemes (Mayo & ESC) one thing is clear. Pulmonary hypertension is the key hemodynamic expression of HFpEF. It could be either resting and persistent or exertional and transient.t is obvious the PH in HFpEF is post-capillary. (The modern term for pulmonary venous HT). Mind you, while PVH is mandatory to diagnose HFpEF, PAH (precapillary ) is also observed in most patients with significant HFpEF. This is the reason TR jet velocity is included as one of the criteria. (To make things simple, we may need to create a new classification of HFpEF, ie resting vs exertional HFpEF.This is what the diastolic stress testing is all about.)
Final message
It is back to basics & time to dig into the fundamentals, of what exactly we mean by heart failure. Is the elevation of LV filling pressure alone sufficient? Should it happen at rest or at exertion, and whether neuroendocrine activation is necessary? Is RASS activation similar in both HFrEF and HFpEF? Try to find the answer to this. How often does HFpEF fulfill Framingham’s criteria of HF.? ( Löfström et al ESC Heart Fail. 2019)
Trying to understand the nuances of HFpEF, I think, we can make a statement,- HFpEF can not be diagnosed without pulmonary hypertension. It makes a lot of sense the P in the H2FpEF scoring system denotes PH, however, It is assigned only a single point, which needs revision. In fact, there is a strong case to argue and make it an essential criterion.
Paradoxically & curiously HF with reduced ejection fraction (which is the most common form of HF) doesn’t require the presence of PAH to diagnose it. This issue may also be examined.
Reference
Posted in Uncategorized | Tagged criteria for hfpef, esc guidelines on hfpef, HFpEF |
Does the Aortic root contract or relax during ventricular systole? Some time back, I asked this question in one of my classes for the fellows and found no takers. Not even a guess? I realized later, it was indeed a tough question. The heart is not the only dynamic organ, as we generally believe. The entire aorta which is an extension of the left ventricle has to be dynamic according to the physics of ventricular-arterial coupling and the momentum of blood flow.
What happens to the aortic dimension with systole?
Even prior to systole, there is evidence, the aorta gets ready to receive the blood from the LV. So, the Aortic root must be larger at the onset of systole. (Ref 2 ) It is been generally agreed now, that the systolic dimension is slightly more by a few mm. That is why aortic dimensions are measured in peak systole as per the American society of echocardiography.
There has been an opposite argument as well. The diastolic aortic dimension could be larger, as the aortic valve is in the closed position and the aortic root distended, & becomes a reservoir of blood that’s meant to be distributed during diastole. What determines the aortic dimension on a moment-to-moment basis? Is it the, LV contractility, pressure, or volume, or the compliance of the aortic wall that determines the aortic dimension and pulsatility? How does a prosthetic valve alter this?
So, what exactly happens to the aortic dimension during the cardiac cycle ?
A wonderfully done study from University Medical Center Utrecht, The Netherlands throws some important facts with their analysis of ECG-gated CT scans in 108 Aortas.(Ref 1)

Clinical implication of aortic pulsatility
The implication of knowing (or not knowing )the dynamism of the aorta can be huge.
- Age-related stiffening and onset of systolic hypertension
- Aortic diameter, pulsatility, and shear stress are the key parameters in initiating dissection and its propagation
- Choosing the right sized valve for AVR
- Current interventional heart-throb TAVI involves just a passive placement of the valve in the aortic root. Imagine what will happen, if the foundations are excessively dynamic and shaky
It is surprising, even after decades of vascular research, we lack clarity on what exactly happens to aortic root during various phases of the cardiac cycle. (Currently, paravalvular leak, & migration of TAVI remains a major worry, which has a direct relationship with pulsatility of the aortic root ) One thing is obvious,.Young cardiologists have a lot of work to do in this arena.
Final message
Though the aorta is a direct extension of LVOT, its vaso-motion doesn’t seem to be in complete sync with the cardiac cycle. It tends to have an independent behavior, out of phase with the heart.
As per available evidence, the aortic root dimension can either increase, decrease, or be static in response to LV contractility.
Reference
2. Pang DC, Choo SJ, Luo HH, et al. Significant increase of aortic root volume and commissural occurs prior to aortic valve opening. J Heart Valve Dis. 2000;9:9–15. [PubMed] [Google Scholar]
3. Vesely I. Aortic root dilation prior to valve opening is explained by passive hemodynamics. J Heart Valve Dis. 2000;9:16–20. [PubMed] [Google Scholar]
Posted in Anatomy of heart, Uncategorized | Tagged aortic root dynamism, cardiology research topic |
Welcome to Kuna island. The Kuna Indians are really unique people. living off Panama, right in the isthmus connecting North and south America, The Kunas reside in the San Blas archipelago comprising about 360 islands, of which about 60 are populated by them. They have lived on these islands for centuries, but their exact origin is not completely understood.
These innocent tribes have taught an important lesson in human blood pressure regulation, vascular biology, and salt sensitivity. We know, that high blood pressure, is a maximally researched entity in medical science in terms of etiology, vascular effects, and its control. Still, we don’t know, what are the limits of normal BP for human beings. The debate will not end until we are clear about, whether human beings evolved from monkeys or emerged as de-nova organisms. Recent studies have revealed a remarkably low level of mitochondrial gene diversity in monkeys, suggesting that there has been remarkably little genetic admixture. (Ref 2)
What we know from 3000-years-old human history is, blood pressure is directly related to the physical work done by us and the diet we eat. While salt is considered pro hypertension, physical activity is a much more important determinant in bringing it down. Normal BP in a pre-civilized world was low compared to a civilized population. They also enjoyed better vascular health. Where is the evidence? It comes from the life cycle of Kuna Indians. Here is a very unique paper published in the Hypertension journal.(Ref 1) Three cheers to the authors for confirming this long pending speculation with meticulous data collection. (See the Image)
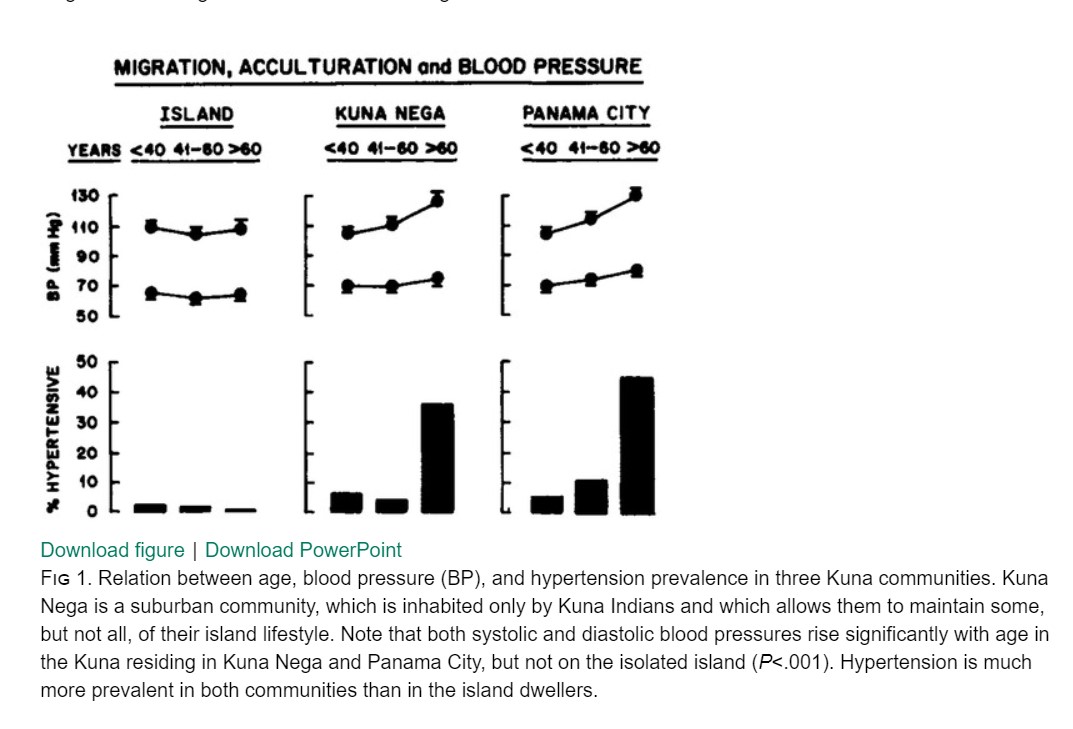
What was special in Kuna’s diet that prevented cardiovascular events? It is been shown in the study by Hollenberg, their diet contained rich in cocoa and flavonoids that made the difference.(The salt consumption was still high though)
As Kuna’s moved out from their primitive lifestyle to first, the Kuna Nega,(a suburb) and subsequently to a fast-paced Panama city. See the impact on their systole and diastolic stress on the heart. The loss of protective effect of the native diet is obvious.
Final message
Lifestyle is the buzzword today. It is a by-product of the new civilized world that will define human health. The human vascular tree tries to sync with a new lifestyle pushing the BP curve to the north. The true normal BP for denova-human beings may still be very much lower than what we believe. A crazy suggestion was made, that human BP should match that of non-sedentary monkeys. I Hope, we get more evidence later for such hyperboles. As of now, we have to accept, hypertension is largely due to disorder in human civilization, development, and prosperity.
How about embracing the styleless lives of native Kunas to take control of our vascular health.
Reference
BROWN (S.), ATKINS (C.), BAGLEY (R.), CARR (A.), COWGILL, DAVIDSON (M.), EGNER (B.), ELLIOTT (J.), HENIK (R.), LABATO
(M.), LITTMAN (M.), POLZIN (D.), ROSS (L.), SNYDER (P.), STEPIEN (R.) – Guidelines for the Identification, Evaluation, and
Management of Systemic Hypertension in Dogs and Cats. J Vet Inern Med, 2007, 21: 542-558
Posted in Uncategorized | Tagged kuna Indians and hypertension |
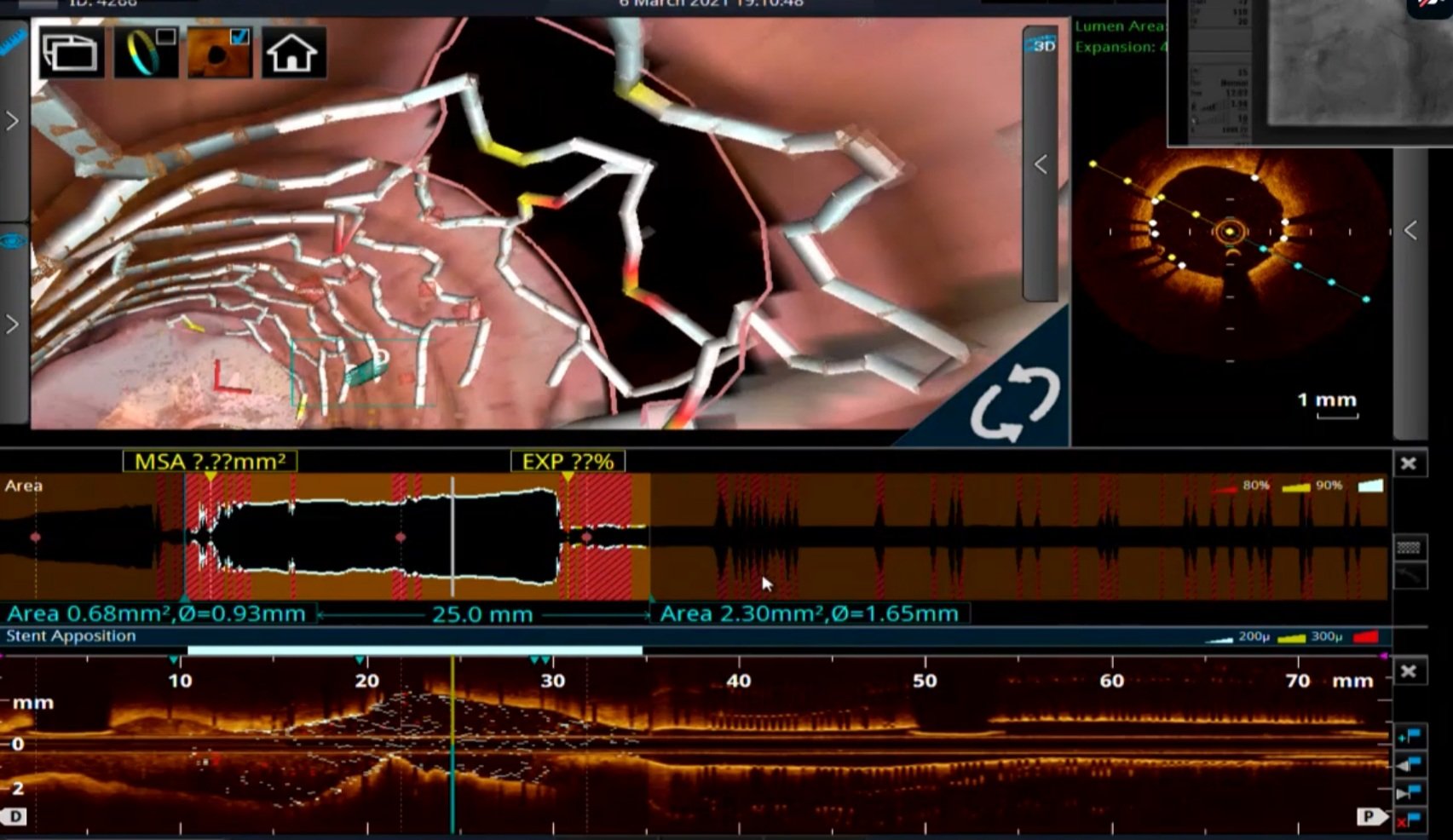
This is the story of PCI to LAD from the customary bifurcation workshop for the budding experts, which ended up with a compulsive final OCT run-through, triggering a debate on what to do with the side branch.
- Just balloon dilate the distal strut
- Would consider a second stent. Maybe a TAP depending upon LCX morphology
- At this stage, I would like to know the FFR or iFR across LCX Jail.
- Get rid of this OCT, Let me have look at regular CAG. I bet I can make a better decision.
- Leave it alone if the clinical status & profile is good
Leave it alone? Is it not an incomplete Job?
Definitely incomplete. Please realize, No job is complete in interventional cardiology. If we believe so, it exposes our Ignorance ( & some arrogance). Intentional side branch jailing is an integral part of PCI techniques. Are we not ignoring day in and day out.
Someone in the audience asked Why did you do OCT at all?
The chief operator quipped “You can’t ask this silly question in a scientific workshop. We bought the OCT kit to improve the quality of PCI. We are proud of it. Really feel blessed to use it and I am sure my patients will benefit from it”. We have to agree with him. These new Imaging techniques though give us extra high-definition, but it comes with troubling revelations with their new vision. If you are pathologically honest and believe in empowering patients, it is absolutely necessary to convey the following facts in the discharge record as well. It would be something like this, “There was a 120-micron strut crossing the LCX ostium, that might continuously impede a chunk of platelets & RBCs every beat, for the rest of your life and might enhance the risk for thrombosis. (Of course, DAPT will take care of it and ask the patient not to worry)”
OCT: One-minute review
OCT is Indeed a stunning Innovation. It can be useful in all 3 phases of PCI. 1. Assessment and preparation of lesion bed. 2. during stent deployment and optimization. ,3. Post-stenting follow up. The technology has grown so fast, now angiographic co-registration and longitudinal frame reconstruction comes inbuilt. It required 3 versions of LUMEN study and a 4 th one (LUMEN 4 ) is yet to come, expected in 2022 to prove the worthiness (or worthlessness) of OCT.
One attractively named DOCTORS study asked the specific question directly (Does Optical Coherence Tomography Optimize Results of Stenting)” This is from NSTEMI patients .read yourself for the conclusion. It is not convincing to me. DOCTORS study (Does Optical Coherence Tomography Optimize Results of Stenting)”. Circulation 2016; 134: 906.
Mind you, OCT is not only an expertise-dependent procedure, it also has important imaging limitations. It has low penetration max 2mm, can not differentiate lipids from calcium, shadowing behind red thrombus is an issue and most importantly it may miss the external elastic lamina (EEL) and measurement errors are real.
Cost-effectiveness
If an imaging technique to assess a stent *(*Still waiting to prove its worthiness) could cost more than the device itself, realize how good our economic intellect is. Just because your lab has an OCT console, it need not transform into a technically perfect PCI. There are at least half a dozen factors other than Imaging that matters.
Final message
OCT is a breakthrough technology that needs to be used judiciously and it definitely helps us understand the nuances of coronary stenting, especially in complex lesion subsets, and its mechanical and histological contents. However, let us not propagate a false message, that without OCT we can’t perform a perfect PCI. Give due respect to all those sharp-eyed interventional cardiologists with good techniques, who can do a better job, beating the HD vision of OCT, with their native blindness.
Reference
Post-amble
Can you guess how many PCIs are done with OCT guidance globally?
It is less than 5 %. In India, it must be, I guess it is < 2% So, we are living in a terrifying world of coronary interventions, where 98 % of PCI is happening blindly, sub-optimally, and unscientifically., Data from CLI-OPCI registry adds more panic: Centro per la Lotta Contro l’Infarto – Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) registry: It says device-oriented cardiovascular event (DOSE) is high with OCT detected sub-optimal PCI.
So, what are we going to tell our patients who will undergo PCI (undergone) without OCT guidance in the past, present, and future?
Simply ask them to forget this OCT stuff. Just reassure them. Nothing will happen.
Posted in Uncategorized | Tagged coronary Imaging, ILUMEN study, oct, opitical coherence tomography |
It brings a unique sense of greatness and gratitude to hear the voice of the father of Interventional cardiology decades after his demise.
The invention he made has evolved so much. Though, Dr. Gruentzig didn’t live to see any of them, the genius in him predicted most of them. This Interview was recorded a year before his small plane, which he loved next only to his pet balloons, crashed on the Atlantic coast along with his wife. That is history.
This is how the news was reported across US media on October 29th, 1985. (Reconstructed, click over the pic for high resolution)
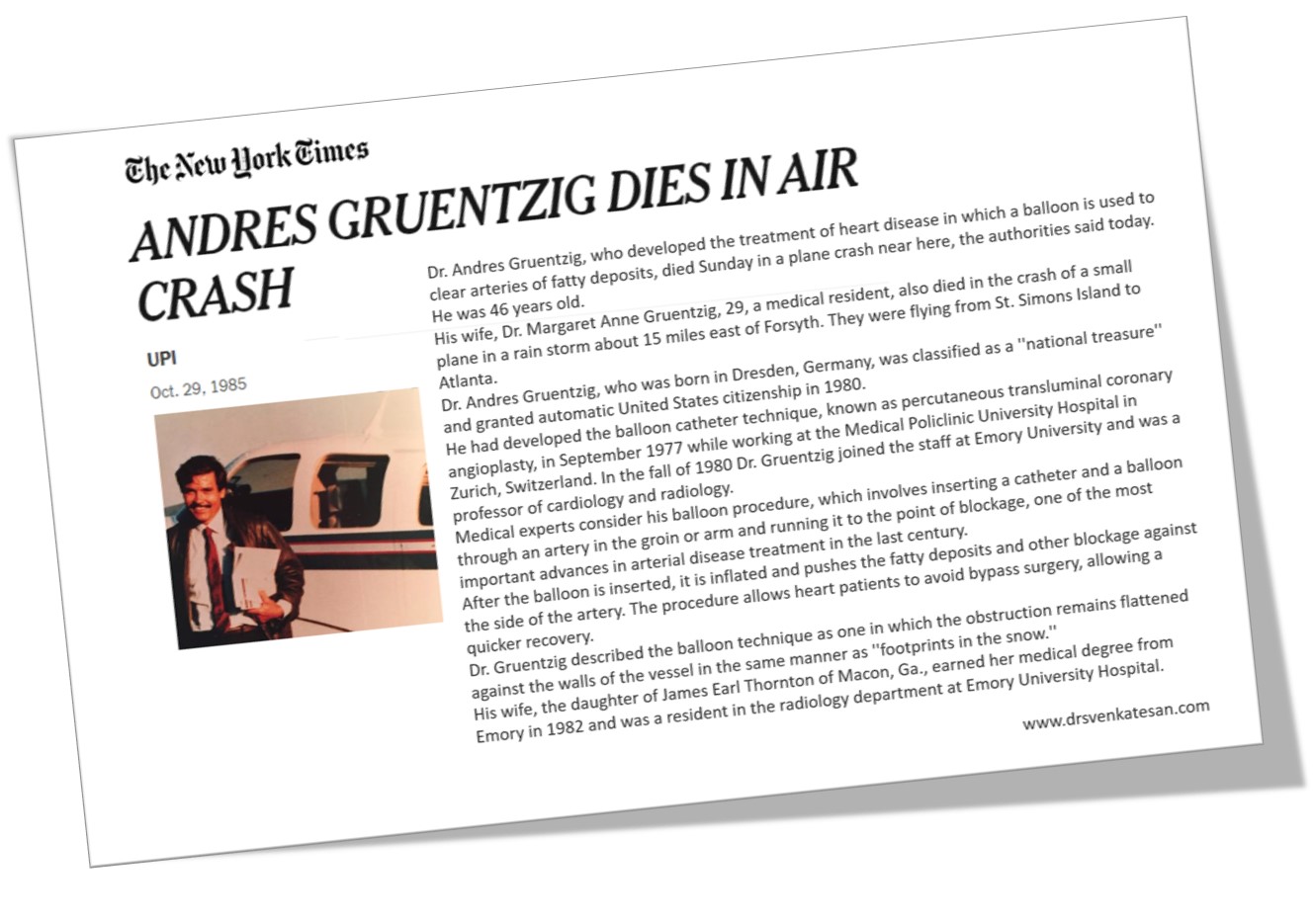
It was a fact, that he defied the warning and flew in the adverse weather, what many of us were unaware of was, that he wanted to rush to Emory, only to see a patient whom he had done a PTCA, a few days earlier, developed some complication. This makes his death all the more poignant (Ref Dr. H.V. Anderson )
Here is a good account of the life history of Dr Gruentzig. Link to the article
Posted in history of cardiology, Histroy of medicine | Tagged Dr Gruentzig, history of cardiology |
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- March 2026 (6)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,635,562 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

