In a population‑based perspective, both paroxysmal and chronic atrial fibrillation bothers us more because of stroke risk than hemodynamic instability. AF confers a 3–5‑fold higher stroke risk and accounts for roughly 1 in 5 ischemic strokes overall.
Stroke‑related disability, recurrent events, and higher mortality make thromboembolic risk the dominant public‑health concern.
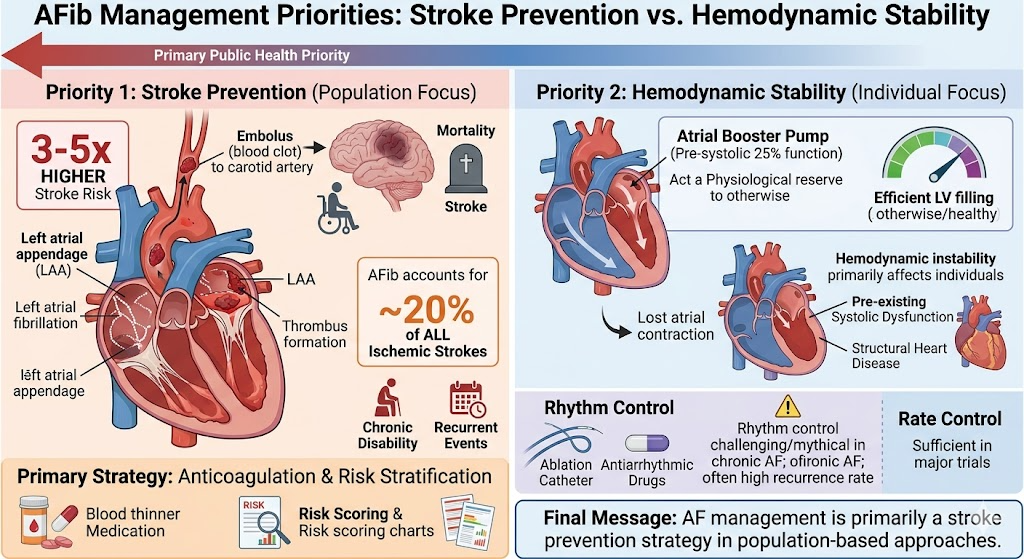
Hemodynamic instability does matter ,in ACS, pre‑existing systolic dysfunction or structural heart disease. At a community level, , stroke prevention (anticoagulation, risk stratification) outweighs rate‑rhythm control as the primary priority. This is exactly the reason, rate control was suffice to beat rhythm in major trials with a optimal anticoagulants.
*The pre-systolic 25% booster pump function acts more as a physiological reserve . We have infinite number of pateints with lone AF , effectively managing the lack of atrial contraction , by the newly recruited LV suction force ( intriguingly, it can function in pre-systole as well )
We must also realise, the much hyped rhythm control modalities actually plays a hide and seek game in many paroxysmal / persistent and most chronic AF . This applies to all sophisticated ablation stuff including the Cryo and PFA. Also, we need to understand stroke in elderly , is not fully prevented even if SR is restored in piecemeals (of time) because the source of embolus can be elsewhere from ventricle, Aorta, Arch, carotids etc.
Final message
Principles of AF management primarily revolves around stroke prevention , while hemodynamics goes to the background. OAC can perfectly take care of the former in most. DOACs are also playing useful alternate role. Contrary to the popular belief, many , LAA occlusion devices and ablation strategies do not necessarily negate the need for OAC in many elderly people.
Reference