Link to a related post , that might add some sense to the above quote
Posted in Uncategorized, tagged acc aha, best medcial quotes on ethcis, esc, medical ethics, medical guidelines, patient empowerment on March 9, 2026|
Posted in Uncategorized, tagged appropriate procedure, bio ethics, bmj, british journalmof medcial ethcis, clinical decision making, dr s venkatesan, esc, inappropriate interventions, lancet, madras medical college, medcial decsion making, medcial errors, medcial ethics, medical education, medical incompetence, nejm, pateint empowerment, principles of practice of medicine, private vs public health, second opinion, third opionion, venkatesan sangareddi, what ails modern medicine on March 8, 2026|
Getting a second opinion from another expert is a valuable option for our patients when they face a complex decision-making process, especially when a cardiac intervention is advised. No doubt, it is their fundamental rights too.But this could be hard, if the second opinion is sought regarding indication for coronary or interventional procedure.
It is much, much comfortable to concur with the original decision if it is pro -Intervention. (even if it is against your conscience). Vetoing a procedure which was advised by some big hospitals is almost impossible for cardiologists sitting at their office, however experienced they may be. This is because it is sort of going against, the mainstream and defying science as well. Both doctors and physicians are stuck.

I confront such situations often from patients following elite cardiology consults. I had been forthright and genuine and said a firm no or yes to many such procedures . I understood much later, that only a minority of the patients followed my No advice , while invariably they accepted my yes.
After much confabulations , recently, I have made some recalibarations on my values, (decent term for compromise ) despite all the ethical stuff I write in these columns. But, three things I ensure , before giving my opinion which goes against my assessment.
“This procedure is not indicated in the true scientific and moral sense, but 1.If you lack full trust, or 2. If you are not ready to accept the risks of not doing it, or 3. If the fear (of not doing it ), would nag you constantly, then get it done as per the advice of the big guys”.
Final message
Until we acquire the courage to express our true opinion , we certainly fall under the tag of medically incompetent.
Very soon, getting a second* or even third opinion may not really matter. Doctors are silently persuaded to follow the guidelines thursted by big scientific syndicates along with compulsion to go with patient wish & preference.
*Caution and clarification
Second clinical opinion for helping to arrive at a medical diagnosis is of immense value and a great thing to do. In fact, doctors themselves ask for it when they are in doubt. This article is about second opinion regarding the appropriateness of various interventional procedures that is defining modern medicine.
Posted in Uncategorized, tagged acc, aha, bari 2 d, bmj, courage, esc, fear driven pci, ffr, ffr driven pci, guideliens cad, indication 2a vs 2b, indication for pci in cad, insurance driven pci, iscehmia driven pci, jama net work, lancet, nejm, oct, pci, scai, symptom driven pci on March 7, 2026|

Decision making for PCI in chronic CAD continues to be delicate. This is especially true, if the lesion is Intermediate and the plaque vulnerablity is susepcted.
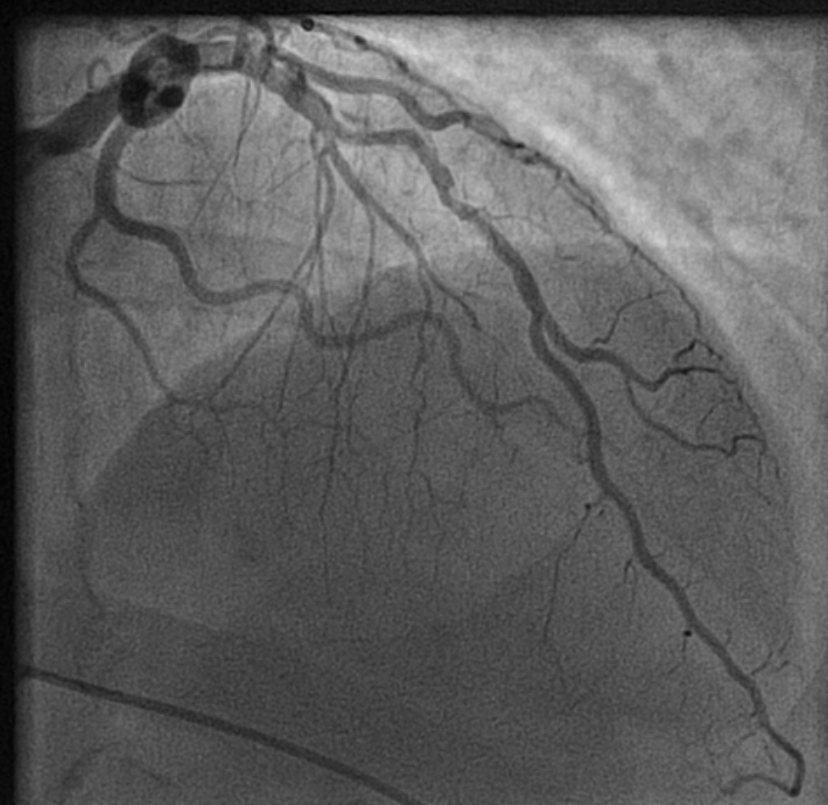
How to tackle this stress positive Intermediate LAD lesion. Functional capacity good. Non-diabetic, mildly elevated lipids. Now, continuing medical management with intensive lipid control is the best possible management. (We have evidence for medical management being good even in significant 90% lesion) Above is a case report from https://www.acc.org/education-and-meetings/patient-case-quizzes/medical-therapy-for-cad
Reassurance is a revascularization equivalent
Sharing a similar experience with one of my patients in his early fifties. After getting a fairly convincing consultation, he accepted medical management. However, guided by both NI & AI, he sought a second opinion to confirm whether my assurance was indeed correct. He underwent FFR and OCT, and both he and his plaque became vulnerable. The FFR was normal. He was too intelligent to ask about the FFR – Stress test discordance, for which his cardiologist had no answer. Still, they did not advise a PCI and the decision was left to him, respecting the current patient-oriented guidelines.
The patient went home empowered but spent sleepless nights, fearing about potential fissures, in the life sustaining fibrous cap.He believed that he was at the mercy of a 75-micron thin cap covering his plaque. In one of the anxious days,in the following week , he got admitted himself in a posh downtown cardiac center. A as per the guidelines, the patient chose his own pathway for a PCI. Cardiologists obliged piously to his wishes. Now, he feels better. He says he is happy to undergo a self prescribed stent.
I was glad, he had the courtesy to come back and showed the results. I learnt. it costed him 6 Lakhs and his insurance covered it fully. I realised , my 30 minutes reassurance was busted by the insurance card in few minutes. I wasn’t surprised.It’s okay, it’s all in the game. I learned it long ago. Fear* (either spontaneous or induced), the power to decide & affordability are the most powerful determinants of any inappropriate medical procedure.
Learning cardiology from UN & WHO
We have United Nations and WHO, the two global guardians. Any one with average intelligence will agree, these instituions can never bring either peace or health to this world.Let us ensure, the practice guidelines of cardiology doesn’t go that way. We boast ourselves, that we have a strongly evidence based vigorously scrutinized cardiology practice framework. How true it is ? Are we hiding behind pateint preference, and pushing science to the background ? Let us be transparent. I think it’s time, the powerful bodies like ACC/ESC should connect all the missing dots. .One important issue is, fear or anxiety-driven PCI, which usually overtakes other true indications.
Final message
In an ideal world , reassurance and GDMT , if properly done, should be a revascularization equivalent in most CAD patients .The reality is, fear* prevails over reassurance, for a variety of reasons.
Postamble
*Anxiety thrives well, in an environment of uncertainty. It is mutually inclusive among both patients and physicians.However most Professional physicians are expected to tackle it. Still many struggle. Patient : What if the block worsens? Physician: What if the patient comes back with an event and oh .. my pride and practice? May be, physicians are not to be blamed much. I think. it is all about a unexplained, biased human mind set. Even a death during an inapproproate Intervention is pardoned off, but an error, raising out of an appropriate medical mangment is rarely forgiven.
Posted in Uncategorized, tagged acc, aortic filter, circualtion research, embol x, esc, innovations in cardiology, ivc filter, laaa occluder, lancet jacc interventions, nejm, PAA-PMF, permanent aortic filter, scai, sentinel device, stroke prevention, TAVR, triguard on December 24, 2025|
“Every Interventional Cardiologist, realistically, need to be a preventive neurologist too!”
The concept a permanent ascending aortic porous membrane filter (PAA-PMF) is an extrapolation of the idea of mechanical thrombus capture, as proven by IVC filters for venous embolism prevention . Also we do have and temporary intra-aortic filters like Sentinel , Embol-X for arterial particulate capture.
The PAA-PMF would feature a self-expanding nitinol frame, with a fully porous head end. The device can be heparin-coated polyester or polyurethane mesh membrane, deployable via 12-14 Fr femoral sheath, similar to IVC filter designs but should be optimized for aortic pressures. Suggested pore size of 100-125 μm targets >100 μm emboli, akin to Embol-X filtration efficacy in capturing 95% of particulates (atheroma, fibrin) during aortic declamping. The essential requirement is that the porous membrane should not create an impedance gradient. How feasible it is, to be tested. Conical shape, the radial force will ensure good ascending aortic wall apposition.
Site of placement is critical. Proximal ascending aorta, 2-3 cm distal to sinotubular junction/proximal to brachiocephalic trunk, as in Embol-X for maximal cardiac/aortic debris interception without coronary/arch compromis
(Only in patients with very high risk of cardioembolic stroke)
1.Chronic stroke reduction in patients with MVR/AVR/TAVR/MAVR
2.High-risk mobile LV mural thrombus
3.Chronic AF with visible and invisible clots in LA
4..High-risk procoagulant conditions with recurrent embolism
*Occlusion and hemodynamic compromise is the most crucial issue. However, when compared to the incidence IVC filter clogging, the high pressure aortic flow is likely to self-wash the device (as happens in a prosthetic aortic valve)
Trapped emboli may enter into coronary circulation is a possibility. Putting a filter at ascending aorta precludes left heart catheterization.
*Migration , Hemolysis are other expected complications.
Intense anticoagulation would be required to prevent occlusion of the filte . (Still, stopping it temporarily doe not not increase the risk of stroke)
Final message : Is it Worth for a Preclinical trial ?
We do have temporary aortic filters. The concept of permanent or semi-permanent filters is largely theoretical, with potential risks being more than benefits. The device can take care of only cardio-aortic embolic stroke.
However, considering so many complex, risky intracardiac and intravascular devices being tested on a daily basis, it is not a big deal for the current generation of interventional cardiologists to try this.
More than our interventional appetite, we really need a device that prevents stroke in a permanent fashion. It is definitely worthy to do initial studies in a porcine model. Would be glad , if Edwards, Abbot or Medtronic and other new Innovators respond to this.
Posted in Uncategorized, tagged aha acc guidlines, cardiology fellows research topic, cardiology research propsal, cardiology research topic, courage, dm cardiology fellows research, esc, fellows research topic, ischemia, non inferiority trials, non-superiority trials, omt vs gdmt, omt vs pci, optimal pci, orbita, pci, PCI VS medical management, ptca, scai, suboptimal pci, suboptimalpci vs omt on February 3, 2025|
The therapeutics of coronary stenosis has become a technogical wonder, interwoven with statistical wordplay in the last few decades. PCI is sitting pretty at its peak glory.The term OMT or GDMT is a popular terminology, but realistically exist only in guidelines.

It is a strange academic habit among cardiologists, that they have subdivided medical management into optimal and suboptimal. Meanwhile, we haven’t seen any papers from cardiology forums that classify PCI according to its quality. How many of use a term like optimal PCI or guideline-directed PCI (O-PCI, GDPCI). Every PCI, by default, is perceived as good by our flawed coronary intellect.
A single patient experience
Let me share a patient consult from a remote town of north India. He is a STEMI patient (1 year old) with mild LV dysfunction and thinning of IVS and anterior wall. His CAG showed a significant looking, yet non-flow limiting LAD lesion without any troubling symptoms. I came to know he had consulted two institutions and was apparently not happy with their approach (In his own words, “They seem to be primarily interested in caging my LAD than listening to me”).

Somebody has suggested my name. He called me over the phone for a consult. I asked him remain there to follow his doctor’s advice. But, he flew some 2000 km to meet me. He was so knowledgeable and was aware of everything I wanted to tell. Like, viability, scars, futility, and benefits of revascularization, imaging-assisted PCI, impact of PCI on exercise capacity, importance of risk factor management, etc.
I told him, “In my opinion, you have technically a single vessel disease that can be managed well with drugs. But if PCI is to be done, it should be done in a proficient manner, as the lesion looked hard and was close to the LAD ostium, trespassing LCX as well.” I stressed the importance of a professionally done procedure with enough expertise and follow-up maintenance care.
He was not entirely satisfied with my response. He wanted a clear yes or no! . I told him, “If you have full trust, continue with the drugs at full intensity and do a stress test after 3 months. otherwise, if you keep getting even the slightest doubt and anxiety over the hidden blocks, go for a stent immediately at a good Institution. (My conscience said the latter half of my advice was unwarranted, but I had to; after all, me too need a protective mechanism)
He left my clinic profusley thanking me. I am not sure , how my consult was useful for him and what he is going to decide.
Academic lessons from this patient.
1.Patient fear factor over coronary blocks may be the ultimate game changer. Cardiologists should try to mitigate this fear and at the least should not be an amplifier to this emotion.
2.Leaving tricky profesionaly complex decisions to the patient, is an easy escape route for us, however it comes very close to professional incompetence. (Of course, we do this on a routine basis, approved by the modern medical guidelines, ethics, and legal system, in the name of patient empowerment)
3.Finally, we can grow a potential research hypothesis. A sub-optimal PCI is non-superior to OMT.It is curious there is no study available to compare sub-optimal PCI to OMT. We must also realize there is nothing called standalone PCI. Without concomitant OMT, PCI is a dud. Every young cardiology fellow need to etch this fact in their cortical cardiac memory. OMT often turns out to be the savior of stents, but the latter ruthlessly steals the credit.
Postamble
I could find one study analyzing suboptimal stenting (Ref 1), but it didn’t compare it with OMT. Suddenly, as I finish writing this, a big fact struck me hard, i.e., even a well-done PCI in sophisticated core labs with meticulous care struggled to beat OMT in a barrage of landmark trials (like COURAGE, ISCHEMIA, ORBITA). What is the big deal to analyze suboptimal PCI vs OMT?
Posted in Uncategorized, tagged acc, accurate neo tavi, aortic valve repalcement, bmj, early tavr nejm, esc, ethics, how end points of a study defined?, lancet, medical statistics, primary endpoints, sapiens core valve, stsscore, tavi, tavr for asymptomatic, tavr vs surgery on January 18, 2025|
We know TAVI is in the striking distance , to literally take over most aortic valve interventions. From a humble beginning from very high surgical risk with prohibitive comorbidity, now it has almost touched the totally asymptomatic, relatively morbid-free patients. Thanks to the hardware, expertise, and motivation from multiple forces.
While the numbers increase, still the debate between SAVR and TAVR is riddled with speculation, skepticism, and absolute confidence. (Reason: TAVI is a passively fixed valve in a blind procedure at a self-selected annular plane, with no option to remove the crushed native leaflet debris and the resultant complications. Lastly, TAVI’s lifespan* is currently less than half of a mechanical valve. *Expected to improve with polymer valves)
The latest trial to join the litereture is EARLY TAVR in October 2024
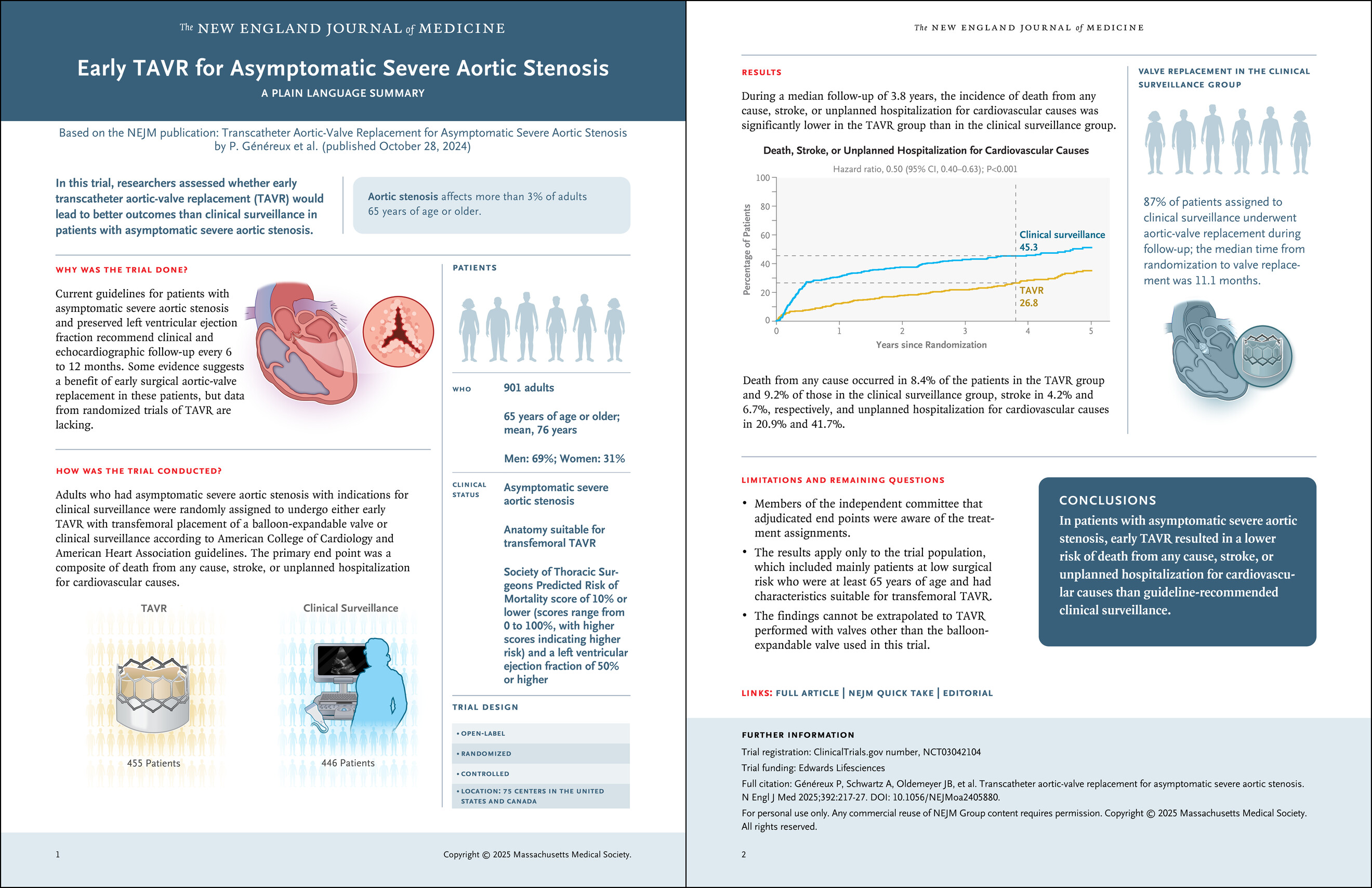
Here is a brief, personal comment about the paper for non-academic consumption. Look carefully at the 15th second of the video. Pause it, look at the number over there on the bar of unplanned hospitalisation.
It is a staggering 41.7% in clinical surveillance group, twice more than TAVI group, pathologically tilting the conclusion of the study.
Video source and courtesy https://youtu.be/3wwQEEG4aWg
By the way, what is that unplanned hospital admission? Who is planning that admission in the asymptomatic control group? If 41% of people in the clinical surveillance group needed hospital admission, what does it mean? Does that mean clinical surveillance was so poor that they were rushed to the hospital despite being asymptomatic and stable in the surveillance period?
Why should totally asymptomatic patients get admitted in the control arm, in such huge numbers? You can presume what could be the reason. My guess is too sinister.
Another issue plaguing the RCTs for decades, is continuing even in 2025. That is putting together death, stroke, and unplanned hospital admission as a combined endpoint in the same basket. This is the familiar old cheat story i.e., used to intentionally torture the truth.
Final message
Any student with basic sense of statisitcs can interpret the result of this landmark trial from NEJM correctly. The question we need to ask is, what are the triggers for those unplanned hospital admissions?
Further, it is good for NEJM (and the medical community) not to accept any papers, if the studys’ endpoints are not appropriate or defined with the intention to manipulate, which happens in many sponsored trials.
Posted in Uncategorized, tagged acc, aha, atorvastatin vs rosuvastatin, avert study, bmj, esc, jamanetwork, lancet, lipid association, lodestar study, lodestar trial bmj, nejm, saturn trial, simvastatin, statins, which statin superior on November 10, 2023|
Statins belong to a group of drugs, stolen and reengineered from the blueprint of natural Chinese red yeast rice (Monocoline K) in the late 1980s. The rest is the remarkable history in the pharma industry.
Statins directly interrupt the cholesterol synthesis by blocking HMG-CoA within the hepatocytes. It significantly lowers the LDL, fights human vascular atherosclerosis. It makes the plaque either regress, prevent progress, make it harder and in the process make them less vulnerable . There are innumerable studies that document the evidence. Statin has become a must-prescribe drug in any one with clinically established CAD or even in concealed CAD. Guidelines are available to prescribe statins various intensity, depending on the risk profile.
Which statin ?
There has been a long list of statins. Many of them have retired from the ring .Currently, the fight is between Atorvastatin, a Rosuvastatin. Like Pepsi vs. Coke.
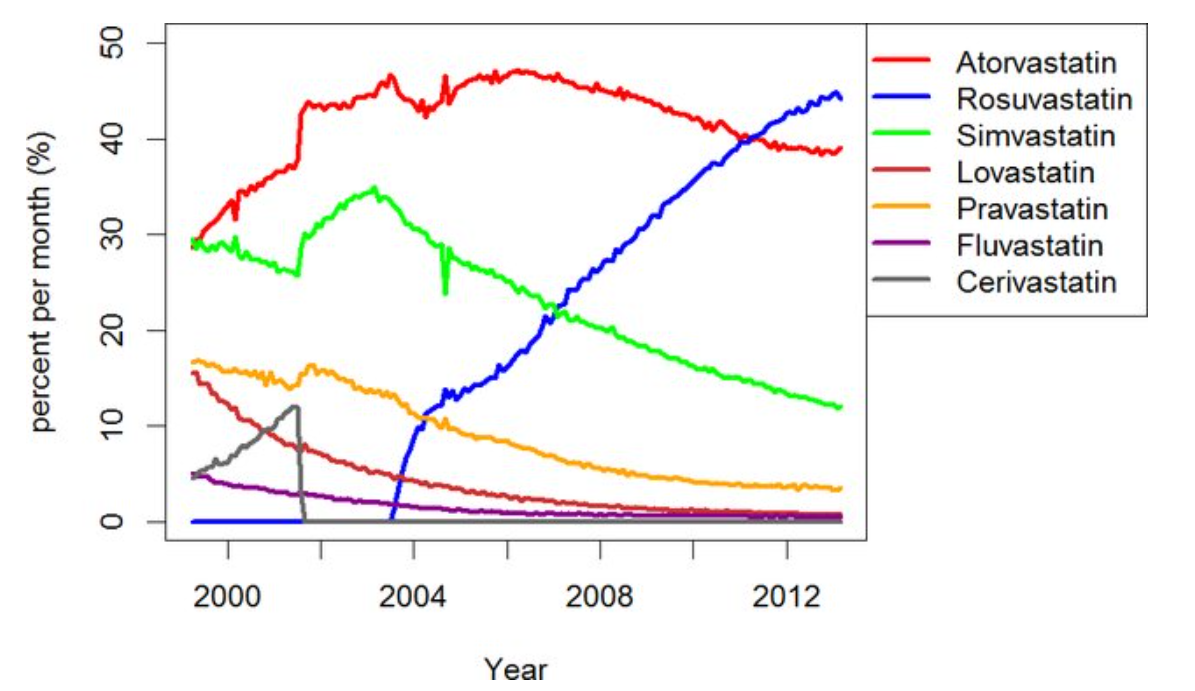
Note the graphic ,A meteoric rise of one drug since 2005 . (Can you guess the reason ?)
ATRORVA or ROSUVA Which one should I choose ?
There is very little “one to one” comparison study between Rosuvastatin and Atorvastatin .The gap in the pros and cons are narrow. Following points are observed, without much dispute.
1.Rosuvaststin is more powerful.
2.Plaque stabilisation effect is not different((Satrun, study NEJM 2011 based on IVUS)
3.New onset diabetic risk is more likely with Rosuvastatin
4.Worsening of cataract is also more with Rosuvastatin
5.Atrovastatin has some additional benefits in lowering triglycerides. (Bakker-Arkema RG, JAMA. 1996)
No one is dare enough to give strong verdict . Surprised to find one this month. BMJ has come out with a possible answer. It is called LODESTAR trial (Ref 1)
Mechanism of new onset diabetes with statins (REF 3)
It can be 7% with Rosuvastatin (less with Atorvastatin). We think, statins act primarily within the hepatocytes where cholesterol synthesis takes place, but they also have an eye on the pancreatic β-cells as well. It down-regulates GLUT-4 in adipocytes, and results in compromised insulin signalling. Furthermore, statins’ impact on epigenetics may also contribute to statin-induced T2DM via differential expression of microRNAs.
Mechanism of cataract with statins (Ref 2)
The cells lining that line the lens are dynamic and require cholesterol on a day-to-day basis. Statins inhibit proper epithelial cell development within the crystalline lens, where cholesterol biosynthesis is critical to maintain transparency and structure of the lens.
Final message
So, is it Atorvastatin or Rosuvastatin? It is left to you.
Mind you, “no statin at all” is the best option if circumstances and risk profile allows. Statins are never considered life-saving staple drugs in our fight with CAD and atherosclerosis. We, along with our scientists might may make you feel like that. Lipids can be controlled within desirable means exclusively with diet and exercise in most of the population* .
(*Forget about statins in the last 5000 years of known human existence, so many great people have lived a long and successful life in this world, without even knowing there is an organ called the heart that is responsible for the circulatory system)
Reference



