The fact that regurgitant lesions are well tolerated in pregnancy, by no -way means, women with stenotic lesions always fare badly. Valves do have reserve excess orifice. This means, it can handle the increased blood volume of pregnancy . A stenotic valve do elevate its gradient from the baseline. This increase in gradient is essentially due to augmented cardiac output and not reduction of orifice size.These elevated gradients sustain the required stroke volume and cardiac index, throughout the pregnancy.
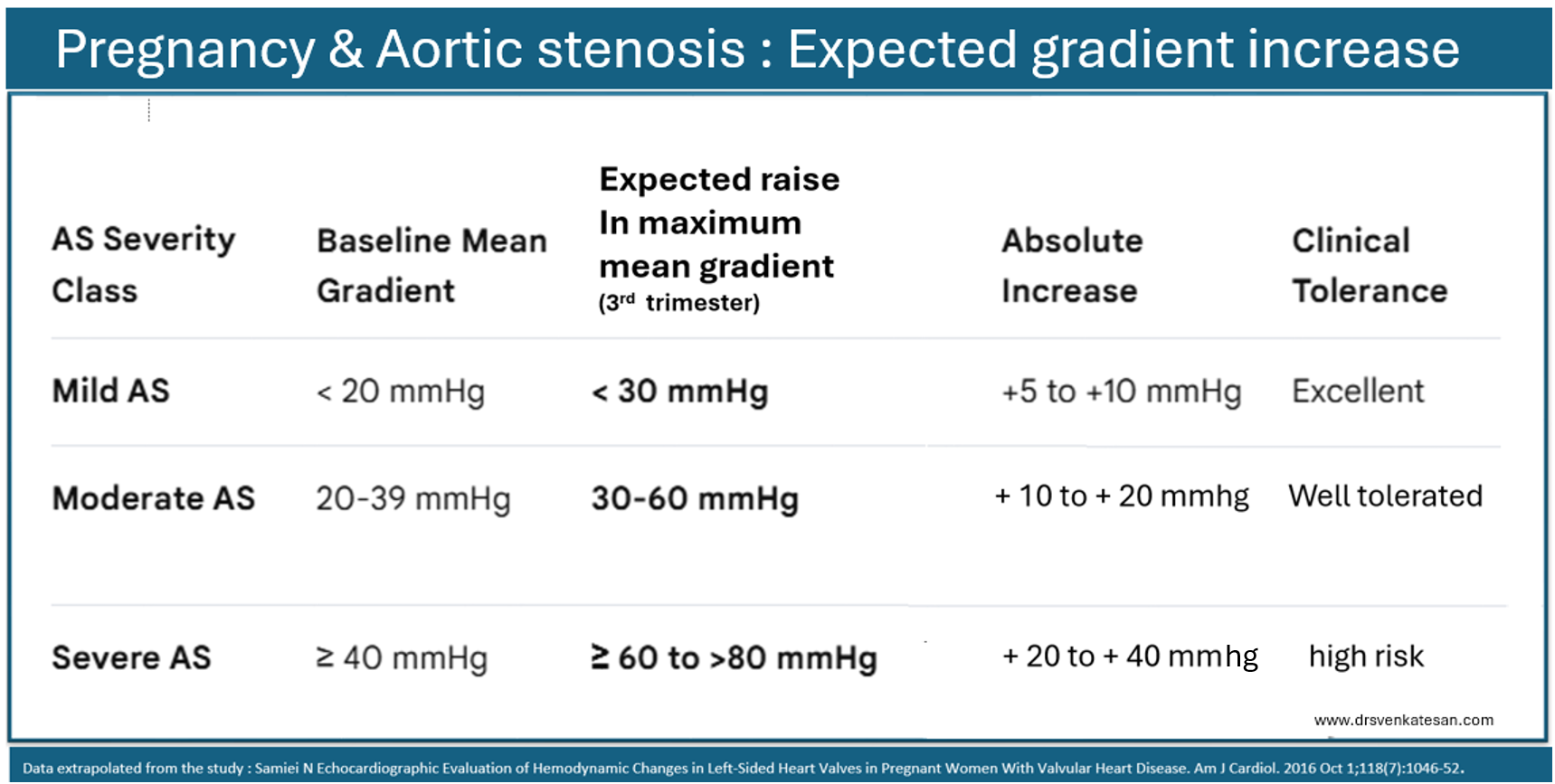
Aortic stenosis in pregnancy
Since , most pregnant women are young, the LV function is good enough to sustain the high gradient. It is also possible, the increase in gradient can be spurious , as it is more to do with Doppler mathematics, as we convert velocity to pressure with a simplified Bernoulli equation.What we really bother about is the stroke volume
The folowing table gives a rough course of Aortic stenosis in pregnancy.
Pregnant women* with heart disease has to cross at-least three hemodynamic hot spots during the tenure. The first task comes around 20 to 24 weeks. The hemodynamic stress almost reaches 80% of maximum. If the mother doesn’t worsen at the end of 24 weeks, it is very likely she will pass through the rest of pregnancy. Another less stressful milestone is around 32 weeks where , she reaches the peak hemodynamic stress. Not to forget, the most critical period (48 hrs) is in the immediate postpartum, where the stress of labor and uterine involution infuses more than 500 ml into the maternal circulation. (*It is not clear whether the blood loss associated with either normal or cesarean section will negate the stress of volume overload. In fact, there is no study that has specifically addressed this issue in heart disease complicating pregnancy. However , PPH always harm the mother.)
Final message
Somehow, we are more obsessed with gradients than what really matters , ie the stroke volume and cardiac output. The fear of high mortality with increasing gradients is more of imaginary. In fact, it tells us about the reserve LV power.Most of the mild to moderate AS is well tolerated throughout pregnancy. Of course, severe AS requires intensive monitoring or a temporary balloon dilatation as we do pre-TAVI procedure. (Or full-fledged TAVI may be considered as a last resort.)
Ironically, in the current hyper-academic environment, more than the true hemodynamic stress of the mother, the Obstetrician’s mental stress is much, much higher when confronted with any heart disease with pregnancy. There are many untold stories, where obstetricians, (Influenced by of new-age cardiologists) are compelled to pursue risky interventions in pregnancy to fulfill protocols & guidelines.
Reference
What happens to trans mitral gradient during pregnancy in mitral stenosis ?
Natural history of gradients in mitral stenosis in pregnancy.
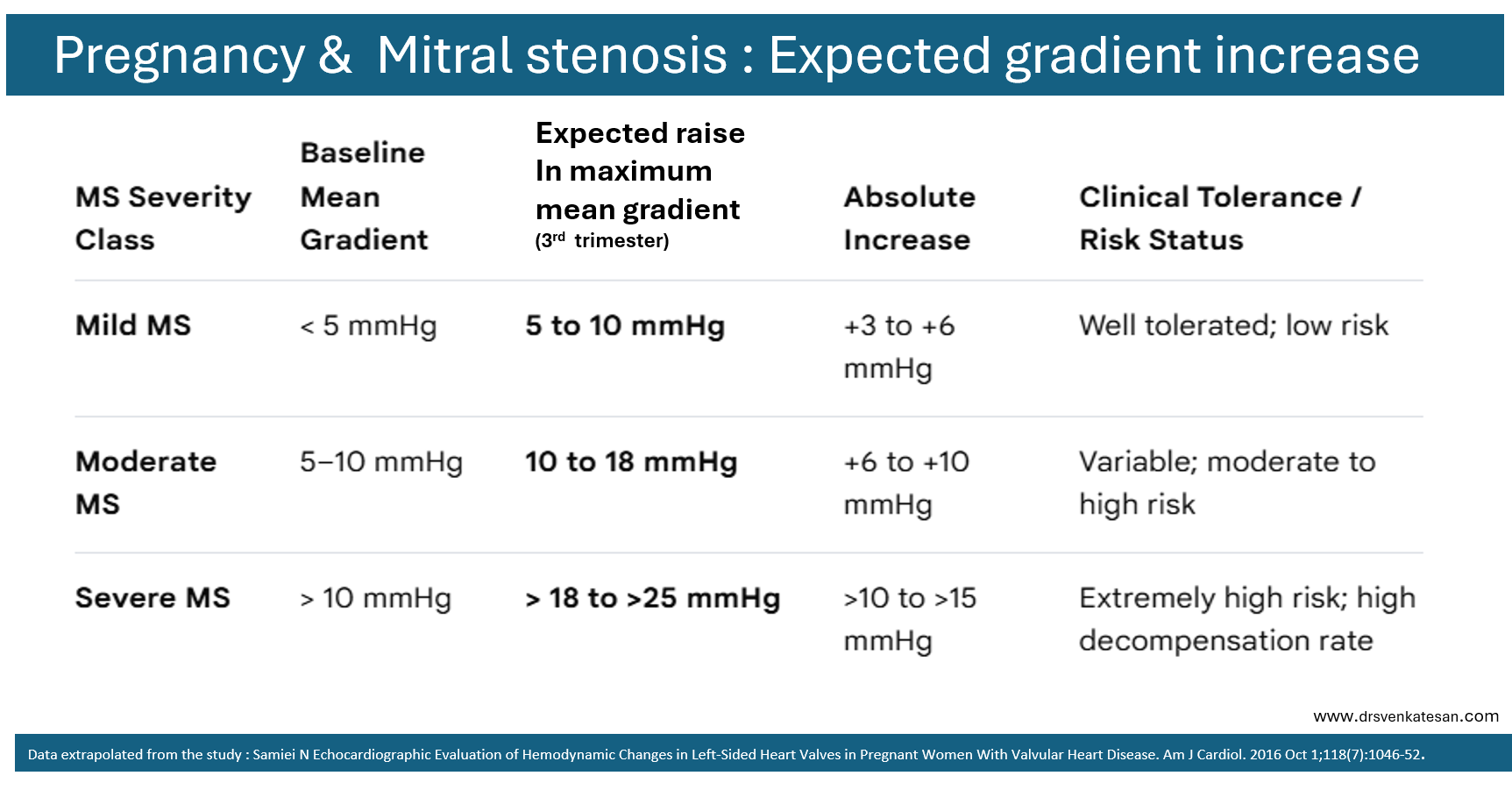
Unlike AS, where the most powerful cardiac chamber of the heart , ie LV is challenged, in mitral stenosis LA has to fight its battle alone, or with help of RV. The risk of acute pulmonary edema is many fold fold high in MS. In countries with rampant RHD, and severe MS, mortality can be high. Still, very selective use of PTMC is recommended in pregnancy even in severe MS .There are numerous case reports of mother and baby crossing the finish line successfully , with the support of experienced obstetrical team (Of course ,this will be called as more of luck though !) The reality is, the professional guilt & fear of not doing a PTMC, often exceeds our confidence, on the resilience and endurance of a young mother’s, compromised heart.



