We know TAVI is in the striking distance , to literally take over most aortic valve interventions. From a humble beginning from very high surgical risk with prohibitive comorbidity, now it has almost touched the totally asymptomatic, relatively morbid-free patients. Thanks to the hardware, expertise, and motivation from multiple forces.
While the numbers increase, still the debate between SAVR and TAVR is riddled with speculation, skepticism, and absolute confidence. (Reason: TAVI is a passively fixed valve in a blind procedure at a self-selected annular plane, with no option to remove the crushed native leaflet debris and the resultant complications. Lastly, TAVI’s lifespan* is currently less than half of a mechanical valve. *Expected to improve with polymer valves)
The latest trial to join the litereture is EARLY TAVR in October 2024
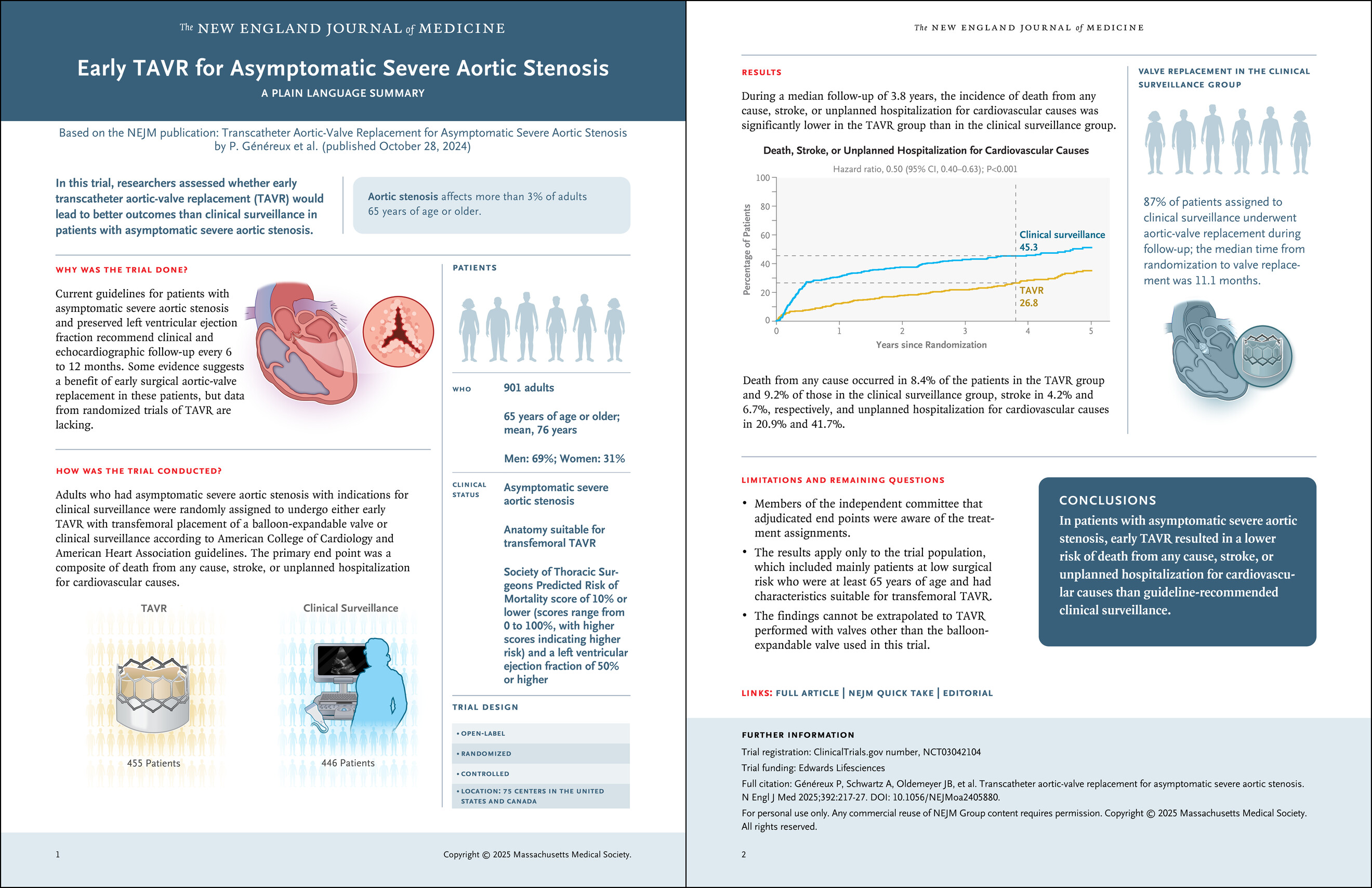
Here is a brief, personal comment about the paper for non-academic consumption. Look carefully at the 15th second of the video. Pause it, look at the number over there on the bar of unplanned hospitalisation.
It is a staggering 41.7% in clinical surveillance group, twice more than TAVI group, pathologically tilting the conclusion of the study.
Video source and courtesy https://youtu.be/3wwQEEG4aWg
By the way, what is that unplanned hospital admission? Who is planning that admission in the asymptomatic control group? If 41% of people in the clinical surveillance group needed hospital admission, what does it mean? Does that mean clinical surveillance was so poor that they were rushed to the hospital despite being asymptomatic and stable in the surveillance period?
Why should totally asymptomatic patients get admitted in the control arm, in such huge numbers? You can presume what could be the reason. My guess is too sinister.
Another issue plaguing the RCTs for decades, is continuing even in 2025. That is putting together death, stroke, and unplanned hospital admission as a combined endpoint in the same basket. This is the familiar old cheat story i.e., used to intentionally torture the truth.
Final message
Any student with basic sense of statisitcs can interpret the result of this landmark trial from NEJM correctly. The question we need to ask is, what are the triggers for those unplanned hospital admissions?
Further, it is good for NEJM (and the medical community) not to accept any papers, if the studys’ endpoints are not appropriate or defined with the intention to manipulate, which happens in many sponsored trials.