This is an ECG which I reported yesterday in my clinic . I thought it was a near perfect example for sinus node premature beat .
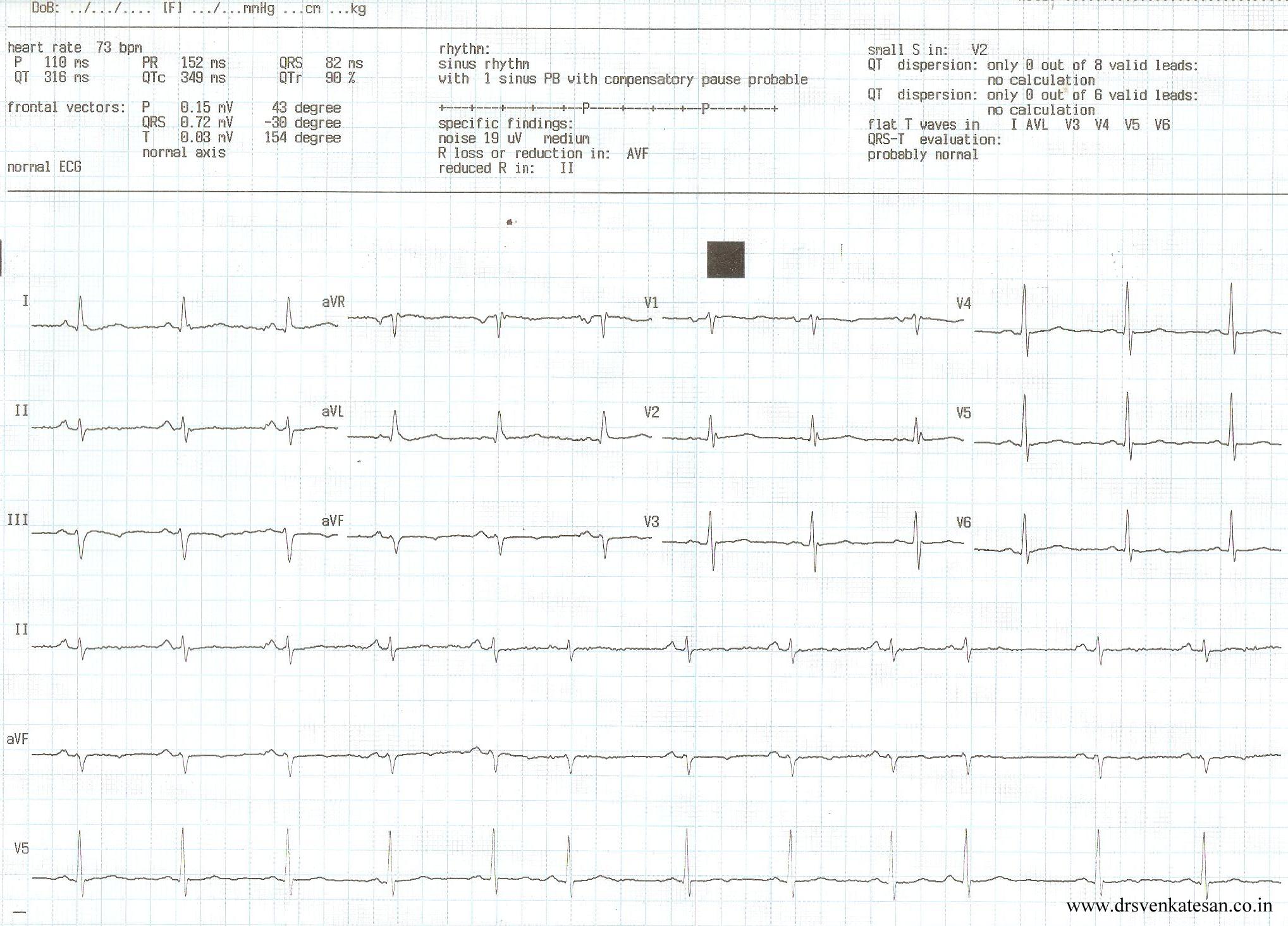
(Of course I need to explain why the P morphology slightly differs )
A sudden unexpected QRS complex is often called as ectopic beat . If it occurs prematurely (ie earlier than anticipated ) it is called as premature beat. If it occurs late it is refereed to as escape beat .Please note the difference is not absolute .
Sinus node is a dramatic bundle of energy with divine powers that drives rhythm of life !
The pacemaker cells are arranged in a compact fashion with differential properties from cranial cells firing fast and caudal cells little slower. The neural control is under constant Neuro/electro/humoral servo control mechanism.It is well known the pacemaker shifts it’s firing location within the SA node in fairly regular fashion .The entire SA node has rich adrenergic and cholinergic innervation , with a dominant control by the later . (This is why the intrinsic heart rate is in the tachycardia range (around 116 ) when SA node is denerved pharmacologically )
SA node , being a complex structure , it is not surprising to note few beats to fire slightly late or prematurely.If it occurs late it is called sinus pause , if it occurs early it is sinus premature beat , if both occurs interchangeably we refer it as sinus arhhytmia. (Read about sinus pause here)
What is the clinical significance of SPD ? (Sinus premature depolarisation )
It is a very benign entity that it is merely an academic fascination . By stretching my imagination I can correlate it with few possible clinical issues.
- May be it has potenital to trigger a SA nodal reentry tachycardia or In appropriate sinus tachycardia/bradycardia.
- It may be imporatnt in sinus node modification process.
- However ,the main issue is thee cardiac physicians in their enthusiasm should not mistake it for some serious cardiac arrhythmia !
Related article
https://drsvenkatesan.wordpress.com/2009/04/14/can-premature-ectopic-beats-occur-in-sa-node/





