Critical and intensive medical care is meant for supporting an individual organ (or multiple organs ) at times of extreme distress , till the healing process prevails over .Later , the patient shall be shifted safely out of the unit .
Whatever be the modern technology , the single most important factor that determines the success of ICU outcome lies within the patient body ( One estimate says patient factor constitutes almost 85-90% -Dukes medical center )
Ironically , the modern gadgets, drugs , devices threatens . . . rather fights . . . with this inherent patient fighting mechanism . We will never-ever know how many cellular switches are turned on by our biological high command , that compensates and tries to restore body homeostasis.

Here is a personal experience with a patient management scenario in an ICU . The patient is none other than my father !
He is a 82 year old man who has developed a acute febrile illness which rapidly degenerated into acute respiratory failure and X ray showing infective bilateral pneumonia and probable ARDS .He was on ventilator for 4 days and subsequently weaned off but still heavily dependent on oxygen . His lung is wet with crackles and wheeze intermittently . His cardiac function was excellent . In one of the episodes of hypoxia he developed , mild shooting of blood pressure and minimal ST changes . Alarmed by this he was started on beta blocker , for the first time . It was titrated up to maximum doses for a suspected ischemic episode .
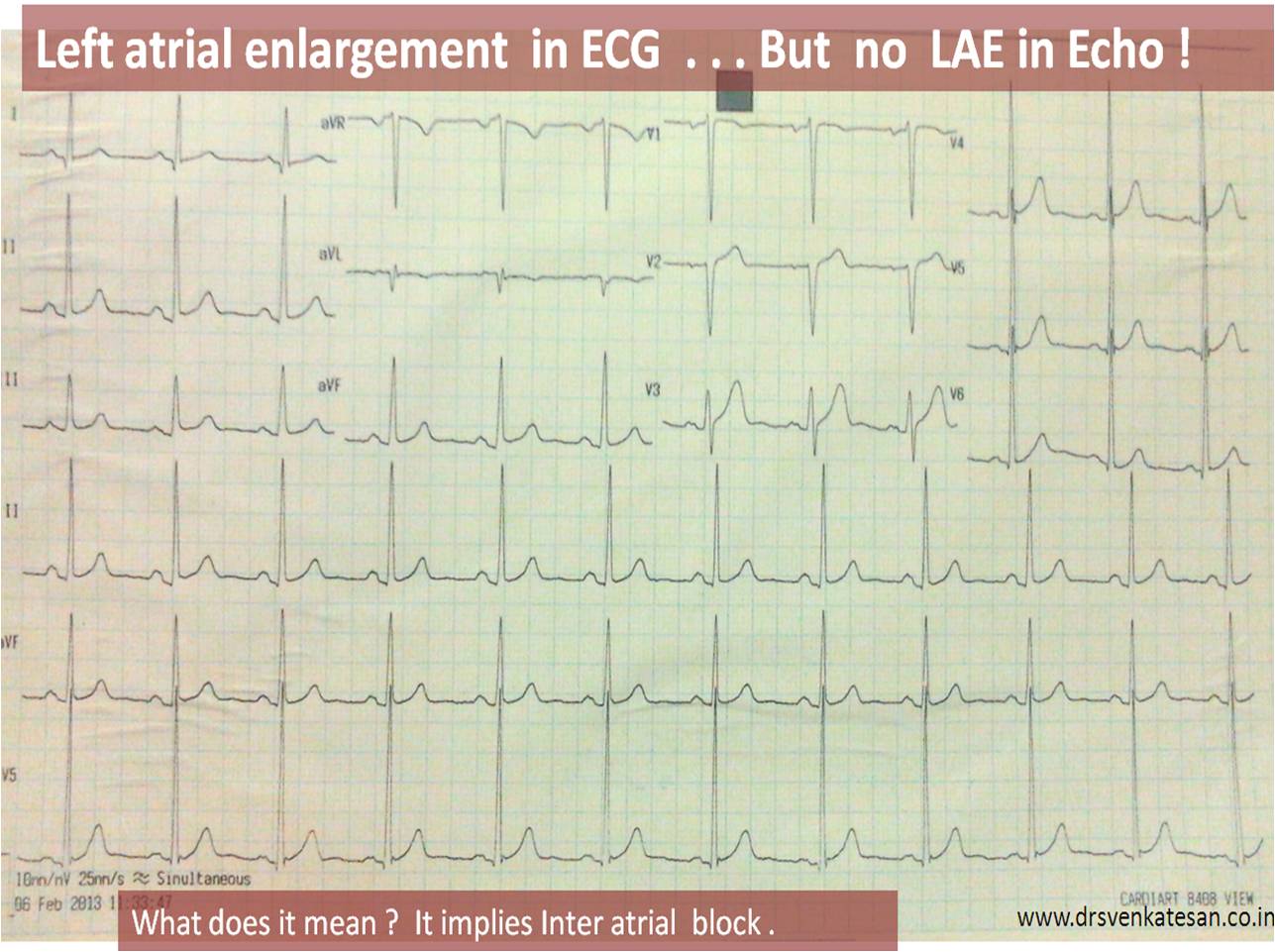
It is well-known , ECG changes are extremely common in hypoxia , tachycardiac stressed individuals .
Sympathetic blockade is important , only if , it is an inappropriate surge . When the body fights a disease it is the only major biological weapon available to him .How is it justified to block it ?
When this was discussed with the team they said they have no power to deviate from protocol and there is one article , that says BBs are beneficial even in COPD !
The patient continues to be in ICU dependent on oxygen with extreme ICU fatigue definitely worsened by the heavy dose of adrenergic blockers which is in my opinion delaying recovery !
Different organ specialist are prescribing drugs according to their level of understanding (evidence is always available for them . . . some where ) and radiology fellows keep taking snaps of distressed organs in various angles in HD quality images . Meanwhile , CT scan seems to have revealed a chronic interstitial process . . . how to diagnose a chronic lung condition in a man who is yet to recover from major acute inflammatory lung Injury ! I do not know ? And the current development is they are considering disseminated tuberculosis !
You may a big physician , the patient may be a very close family member , modern health care system makes you watch helplessly once you hand over patient to a complex care unit .
We hope for the best .
Final message
Medical practice . . . however intensive the care may be . . . the bottom line is . . . it should be based on common sense . Modern medicine tends to make this faculty of our brain blunted .
The specialty of Intensivist is largely misunderstood . It goes more with satisfying scientific egos and public perceptions rather than true patient needs .
We need not react to every changing parameter that emanates from the modern machines that keep sending out live data from a seriously ill patient , on a moment to moment basis ! (We simply do not need that ! If only a pilot reacts with jitters to every air pocket turbulence , he will not reach the destination safely ! )
From a cardiologist perspective , the humble request to all Intensivists and critical care physicians is , avoid being in “fire fighting mode” for all those subtle ECG changes that occur in ICUs , especially with multi- system disorder (Caution : Acute coronary syndrome in CCU / post PCI set up is different story altogether where even a minor ST shift can be significant ! )
Heaven’s sake let us rely more in our brain rather than the machines and devices !
Above story is not even a tip of an Iceberg . I come across it every day in many ICUs I visit . The most saddening aspect is , we can not point out these mistakes to our fellow professionals , as it amounts to hurting academic egos .They are more important than patient care at any given point of time !
Counter point
For any system to work , it needs a strict set of guidelines , other wise the system of care will fail. This is a fundamental basis on which modem medical care works . The only issue is , we should keep checking for any inadequacies in the evidence base and try to correct it. So do not blame the EBM . It has come to stay .That is the future ! You are very pessimistic towards modern science !
Rapid response to counter point
But the real issue is . . . by the time next evidence base finds a major flaw in the existing system of care , damages are already done . So with your clinical acumen every learned physician is free to create his own real world experience .(That is also called Level 3 evidence now ) ** Protocols are not sacred sermons . It may be (rather must be !) violated if there is a need for the benefit of patient .
Disclaimer
* This is not an attempt to disgrace the concept of intensive medical care . Please remember , finding fault could be same as finding facts .(At least in medical care )
Update ( February 24th, 2013 Sunday , 12.05 AM )
After 25 days of intensive and aggressive medical care we lost one of the great lives
of modern times which will be celebrated by his sons and daughters forever !
Read Full Post »