ASD and PDA are almost taken over by cardiologists with device closure. (Including SVC-ASDs) Now VSD is the next target, The pediatric cardiologists are closing in, to conquer it also, except a few large ones and doubly committed VSDs or the ones with poor aortic rims.
Antegrade or Retrograde
The choice of approach between antegrade vs retrograde is gradually getting blurred. The term retro and antegrade often confuses. (At least for me) It may be preferable to use Venous and arterial approach for Retrograde vs Antegrade.
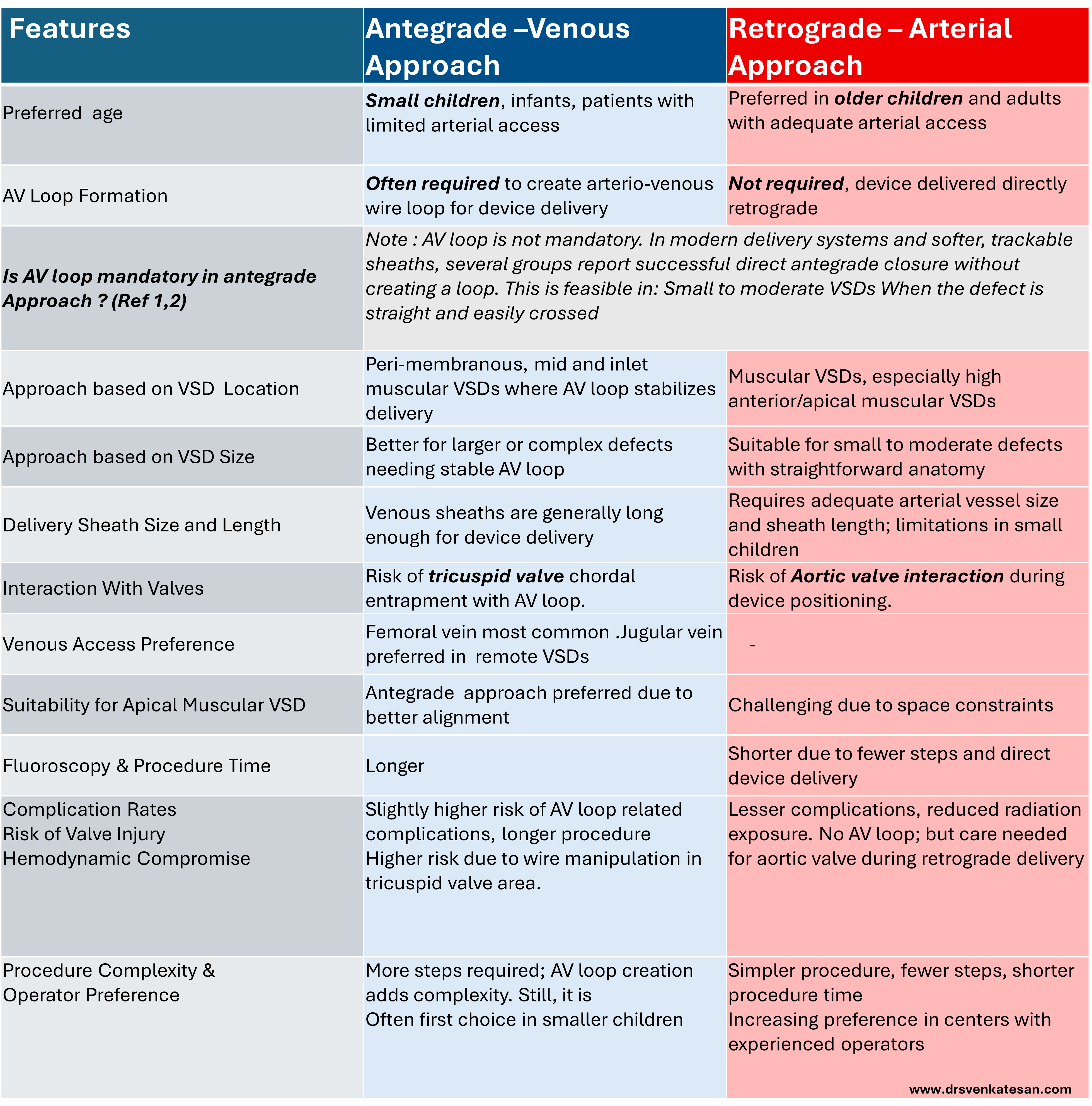
Is AV loop mandatory in antegrade venous approach ?
AV loop is not mandatory. In modern delivery systems and softer, trackable sheaths, several groups report successful direct antegrade closure without creating a loop. This is feasible in: Small to moderate VSDs When the defect is straight and easily crossed .The popular series from Dr .K.Sivakumar & team from Madras medical mission Chennai, India (Ref 1)
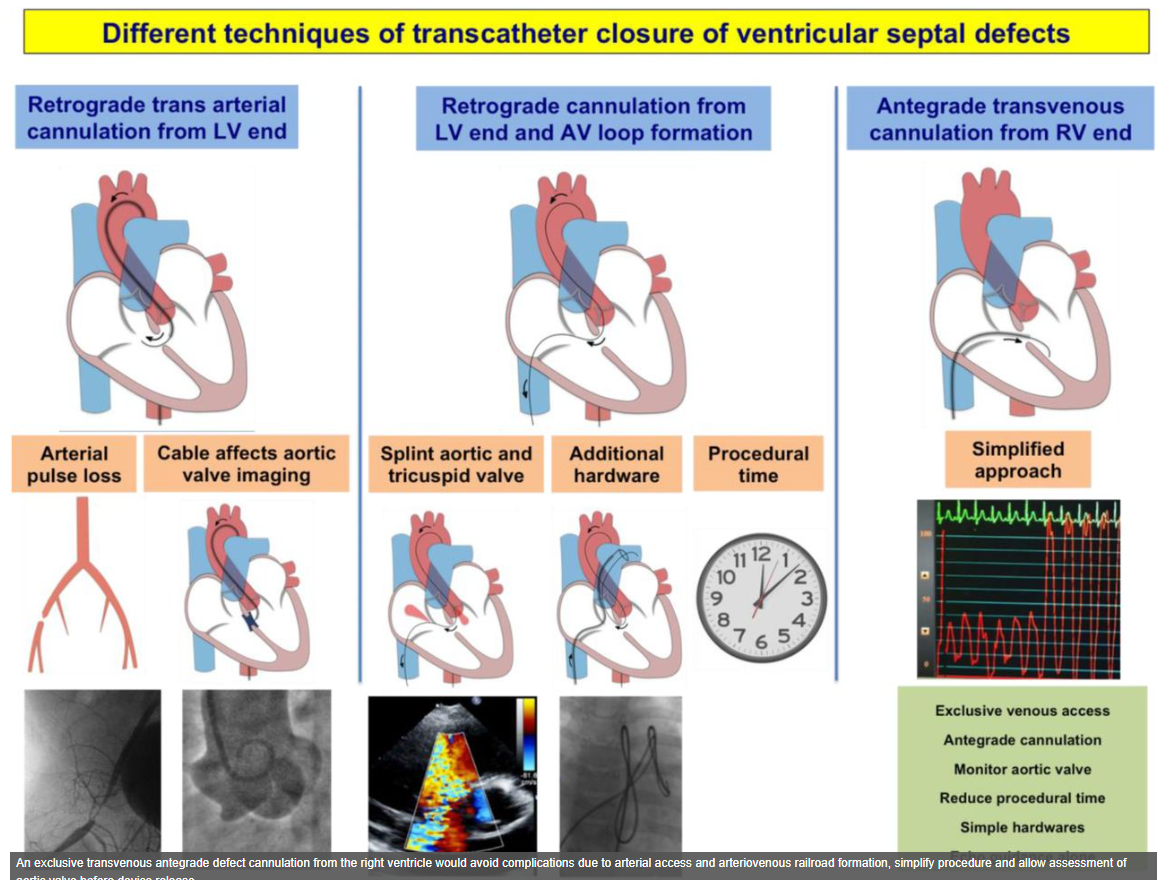
Image source :Ref 1
Reference
- Sagar P, Thejaswi P, Garg I, Singh D, Pradeep A, Dutt N, K.Sivakumar et al. Transcatheter closure of ventricular septal defects by exclusive transvenous antegrade cannulation from the right ventricle: a 5-year retrospective cohort study. https://doi.org/10.1101/2024.05.28.24308078.
- Mehmood DA, Akhtar DK, Kazmi DSSH, Sultan DM, Sadiq DN, Ahmed DA, et al. Transcatheter device closure of perimembranous ventricular septal defect from right ventricular approach without arteriovenous loop. Pak Armed Forces Med J. 2019 May 9 [cited 2025-Sep-19];69(Suppl 1):S5-10. Available from: https://pafmj.org/PAFMJ/article/view/2806pafmj.org
Annexure
Dedicated VSD devices
| Device | Company / Website |
|---|---|
| Amplatzer Muscular VSD Occluder | Abbott – Amplatzer Muscular VSD Occluders product page (cardiovascular.abbott) |
| Amplatzer VSD Occluders (Muscular, Post-MI) | Abbott – Amplatzer VSD Occluders (Structural Heart) (Abbott Structural Heart) |
| Konar-MF VSD Occluder | LifeTech – KONAR-MF VSD Occluder product page (lifetechmed.com) |
| Cera VSD Occluder | LifeTech – Cera VSD Occluder product page (lifetechmed.com) |
| MemoPart VSD Occluder | Lepu Medical – MemoPart VSD Occluder product page (Lepu Medical Technology(Beijing)Co.,Ltd.) |
Non-VSD Devices used off-Label for VSD Closure
These are not designed for VSDs, but can be adapted for VSD. Amplatzer Duct Occluder I (ADO I) Useful for closing large muscular/apical VSDs, especially in infants. ADO II Softer device, low-profile, often used for small peri-membranous VSDs Amplatzer Septal Occluder (ASO) Designed for ASD, but occasionally used in selected muscular VSDs. Coils (Gianturco, Cook, Nit-Occlud PDA coil) can be effective in small muscular or residual postoperative VSDs