Click over the Image for animation

Posted in Cardiology - Animations, Cardiology -Non coronary Interventions -PTMC, cath lab tips and tricks, PTMC -Tips and tricks, tagged difficult ptmc, how to cross a crtical mitral stenosis, inoue balloon, mitral valve crossing, mitral valvotomy, percutaneous mitral commissurotmy, ptca balloon during ptmc, ptmc, subvalvular fusion in ptmc, tough ptmc on October 12, 2013| Leave a Comment »
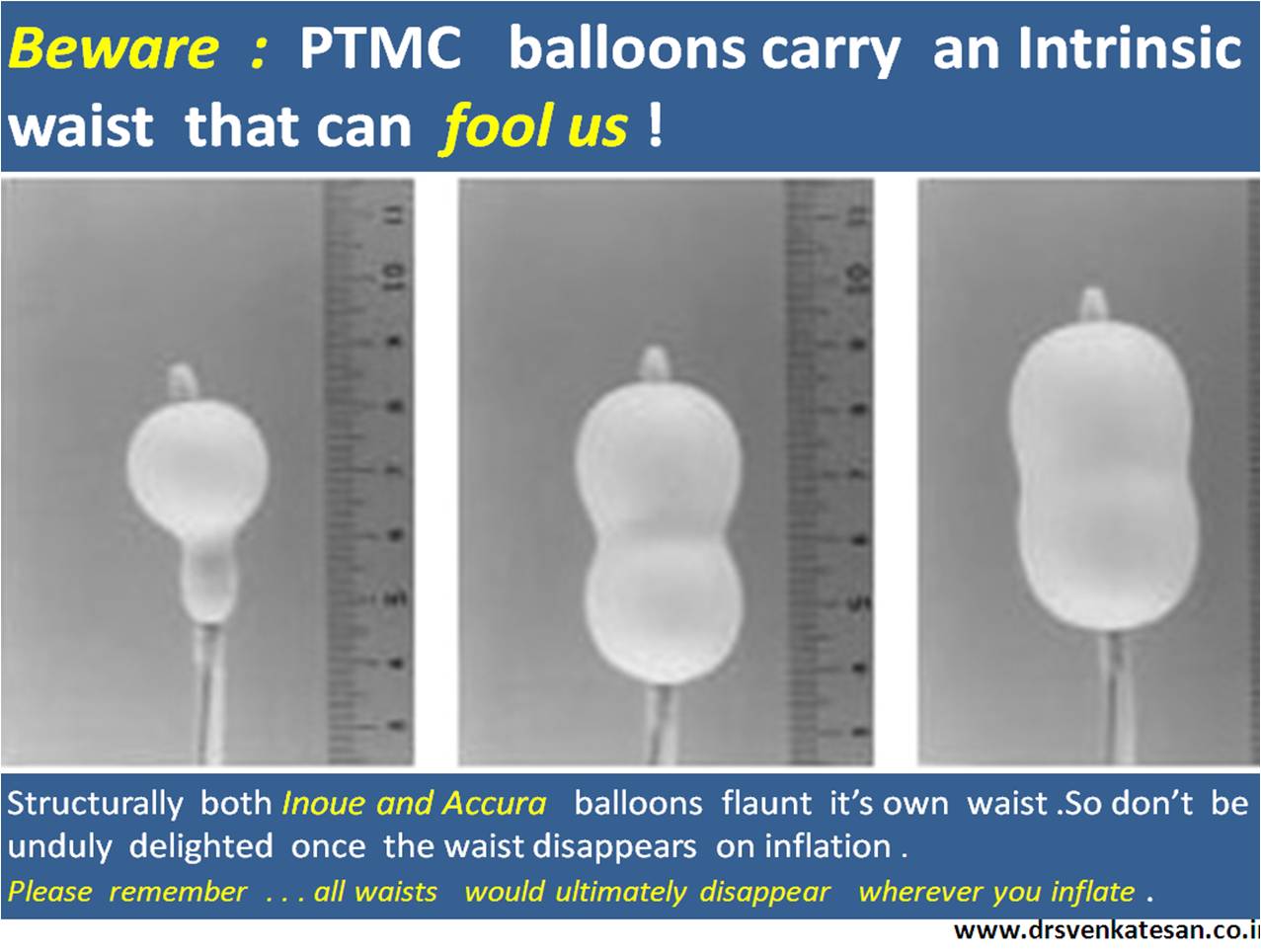
Posted in Cardiology -Non coronary Interventions -PTMC, tagged Accura balloon, inoue balloon, mitral stenosis, percutaneous mitral commissurotomy, ptmc, toray vascualr cocnepts, waist of mitral stenosis on August 12, 2013| Leave a Comment »
PTMC is a revolutionary interventional cardiology procedure .A fibrosed obstructed mitral valve is opened up just like that , with few wires and a balloon .The procedure performed within 30 minutes .No anaesthesia . No surgery .No scar.
Thousands of procedures are done world-wide (Rich countries excluded they do not have RHD) .We in our institute , have gained considerable experience in PTMC , and have completed nearly 200 procedures in the last few years .
As we gain experience surprises also galore ! .Suddenly I realised this funny (At least for me !) phenomenon from the unique PTMC balloon design.
The other day , there was an intense argument between two of my fellows , who were in a dispute .One was arguing , the PTMC balloon had dilated the tricuspid valve erroneously while other was adamant , and wholesomely convinced , since the waist had disappeared it must be the stenotic mitral valve.
The issue came to me . . . ended after a nice debate !
 .
.
Both PTMC balloons (Inoue ,Accura) are made with innovative design conceptualized by Japanese genius Kanji Inoue . The balloon has two layers of latex with a nylon mesh sandwiched in between.The latex is compliant while nylon limits it and generates the required pressure .
The balloon is glued in a such a way , central part is constricted like narrow band .This makes sure the distal part of balloon inflates first , followed by the proximal and finally the central .This also help us to geographically to fix the balloon across the narrow mitral valve orifice .
While , we must agree this a great concept , there is an an inherent issue when handling a hour glass shaped balloon with a natural waist .There would be great deal of confusion when we take disappearing waist as an index of relief of mitral stenosis.
We know ,the key requirement is that , balloon’s waist should match anatomical MVO .But , it is estimated exact match happens in a minority. The issue gets further complex with subvalvular disease , double mitral orifice, eccentric orifices . The efficacy of PTMC is also determined by the appropriate contact of the balloon’s various pressure points . ( It is a balance of intra balloon pressure(3-4 ATMs) and the surrounding tissue pressure !)
Disappearing waists is not synonymous with opening MVOs .All PTMC balloon inflations will shrug of the waist at peak inflation wherever you inflate .(Intra chamber inflations included !)
Final message
Please realise , falling pressure gradients and echo documentation of MVO rules supreme in assessing successful PTMC. Often times , disappearing waist is meagerly an optical Illusion or gratification.



