The primary treatment for end-stage heart failure is heart transplantation, but due to organ shortage and the poor progress in our pursuit for total artificial hearts, LV assist device (LVADs) have evolved from being a bridge to transplantation to destination therapy. Currently, the HeartMate 3 is the leading device in its third generation of LVAD. This fully magnetically levitated centrifugal LVAD reduces shear and thrombosis, outperforming HeartMate II with fewer pump thrombosis events, strokes, and improved 5-year outcomes. Landmark data from the MOMENTUM 3 trial shows that the median life expectancy has surpassed 7 years, with some patients living 9 years or more.
Can LV assist be destination therapy ?
The answer seems be definite yes
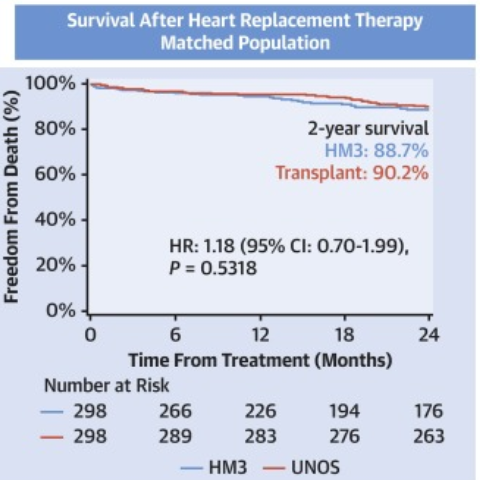
How does it compare with transplantation ?
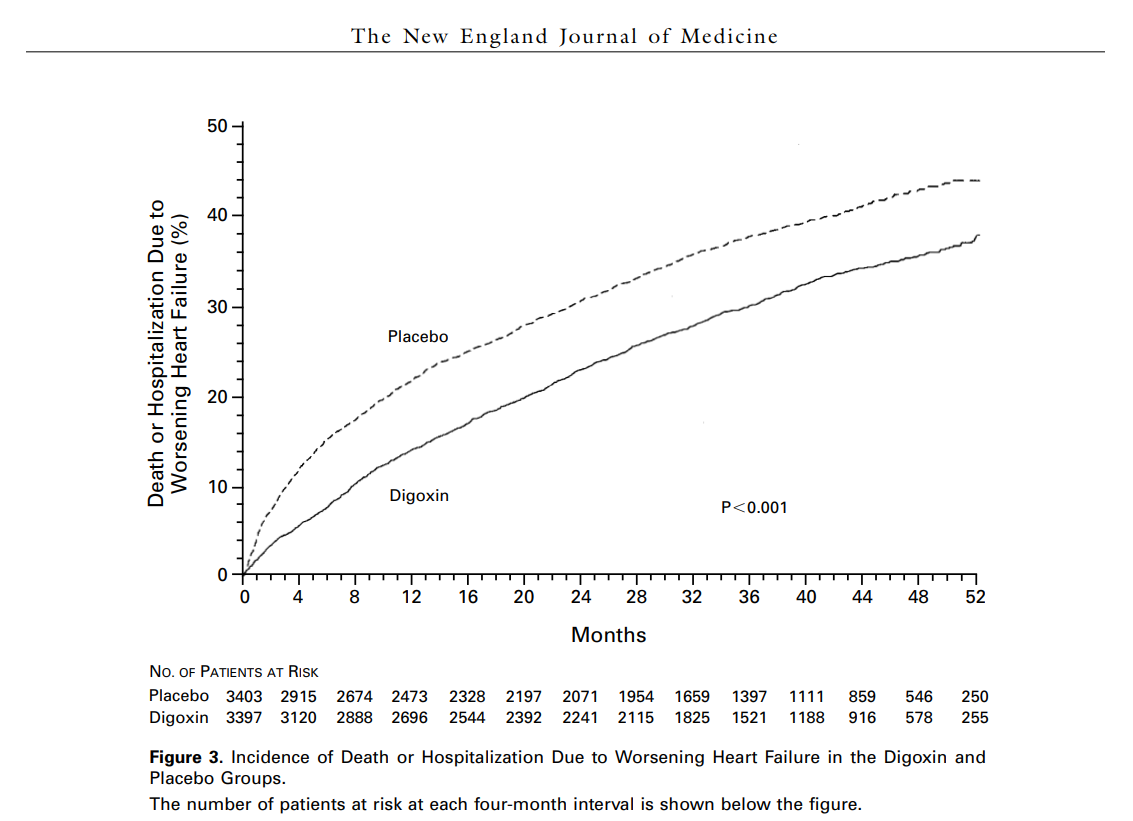
Good , in fact very good for atleast for the first 2 years.See below
How many Heart mates device are implanted world wide every year?
About 40 to 50,000s HeartMate devices are implanted every year
Is Heartmate 3 availbe in India ? Whts is the csot ?
Yes , Heart mate 3 is available in India . The complete surgical procedure and device typically cost between ₹75 Lakhs and ₹ 100Lakhs ($75,000 to $100,000). While cost is one issue , patient’s involvement , commitment , family support is equally or if not more important to administer this therapy.
Is the expertise to mange LVAD avaiable in India ?
The device is available, but expertise in device management is still not optimal , even in large hospitals due to low case volumes.
Any alternative to Heart mate 3?
Medtronic HeartWare HVAD were recalled by FDA for major technical issues in 2021.Another device Eva heart from Japan with a pulsataile pumping technology shows some promise. .Ref Allen COMPETENCE Trial: The EVAHEART 2 continuous flow left ventricular assist device. J Heart Lung Transplant. 2023 .The superiority of pulsatile vs continuous pumps is a different debatable topic )
An illustration about Heart mate .
A true story from a patient on Heart mate 3
Final message
Published studies show that modern LVADs (by default means Heart mate-3) trying to compete with heart transplants. Transplanted hearts has its own un-limited energy to pump ,LVADs are like maintaining a live automobile inside the chest , requiring constant monitoring and energy resource. Also, most importantly LVADs can’t look beyond LV ,and overlook RV function, while heart transplants replace all four chambers, unlike HeartMate, which assists only one chamber.( Of course, isolated LV failure is the culprit in 80% , that’s why LVADs , still could be a good option in many)
Reference
1.Legtenberg S, Ter Maaten JM, Erasmus ME,et al Long-term outcomes of patients implanted with a HeartMate 3 left ventricular assist device-a real-world, single-centre, observational study. ESC Heart Fail. 2026 Mar 3;13(2):xvag074. doi: 10.1093/eschf/xvag074. PMID: 41812231; PMCID: PMC13036835.
3.Boburg RS, Marinos SL, Baumgaertner M, Rustenbach et al Nine Years of Continuous Flow LVAD (HeartMate 3): Survival and LVAD-Related Complications before and after Hospital Discharge. J Cardiovasc Dev Dis. 2024 Sep 30;11(10):301. doi: 10.3390/jcdd11100301. PMID: 39452272; PMCID: PMC11508271.