TAVI has become a popular Aortic Intervention, but the risk of coronary obstruction (Left main & RCA too) is often underestimated , it can happen during the procedure or in the long term .High degree of anticipation is essential. The exact incidence is not known as reporting the event is far less than, what it is actually. Following are the suggested precautions to prevent coronary obstruction.
Pre-Procedural Assessment
- Low Coronary Ostial Height: Identify if the Left Main origin is (< 10–12 mm )from the aortic annular plane, that will increase the chance of struts covering the ostia.
- Shallow Sinuses of Valsalva : A shallow sinus( < 30 mm )leaves insufficient room for the displaced native leaflet, directing it toward the ostium.
- Leaflet Length and Calcification: Evaluate for heavy calcification or a long native leaflet that exceeds the height of the coronary ostium, as these are easily pushed into the vessel opening.
- Virtual Valve-to-Coronary (VTC) Distance: In Valve-in-Valve (ViV) procedures, calculate the VTC distance. A computed distance less than 4 mm indicates risk of coronary obstruction.
Risk factors for potential coronary obstruction.
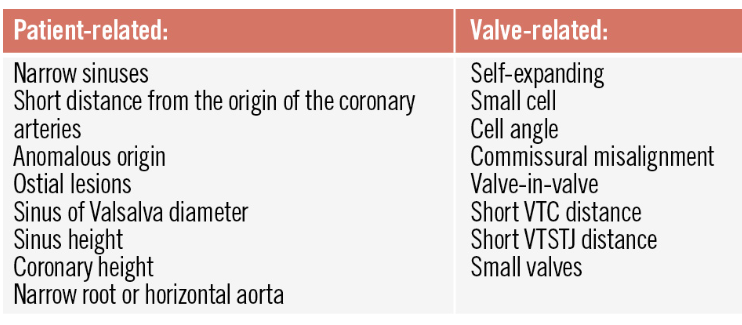
Image source Ref 2
*Leaflet length is a very critical parameter, which was ignored in the past. (It is more Important than even, the coronary height.Mind you coronary height matters little if leaflet is long enough to reach the ostium , when TAVI flushed it with wall of Aorta.)
Intra procedural precautions(In small shallow roots)
- Chimney Stenting: Prophylactic wire in the Left Main and park an undeployed drug-eluting stent. If any segment of TAVI tends to occlude deploy the stent.
- BASILICA/Leaflet Splitting: This is used in ultra-high risk or valve-in-valve cases, use radiofrequency energy or mechanical cutting devices to lacerate the target aortic cusp before valve deployment, forcing it to part like a curtain instead of blocking the ostium.This is not an easy procedure as it may look. Prone for its own complication.
Post-Procedural & Long-Term Management
Dual antiplatelet therapy is critical . Routine echocardiography and follow-up CT angiograms to monitor for delayed coronary obstruction or stent deformation . Documenting the valve-stent alignment is encouraged for a possible future coronary interventions.
Planning a PCI with TAVI
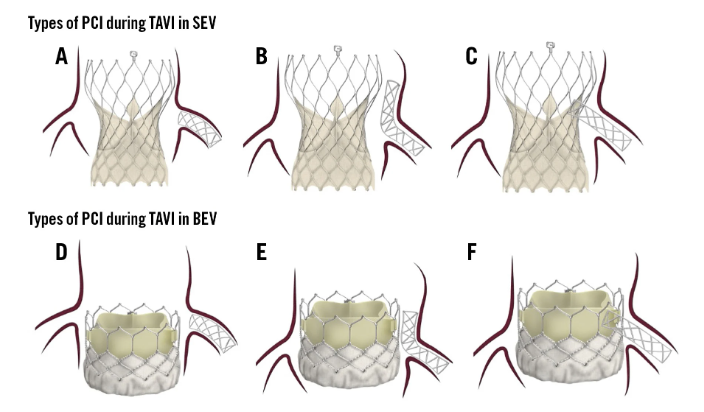
Image source : Ref 2
PCI types in different types of valves. A) PCI with minimal stent protrusion due to limited space between the valve and the STJ. B) Adequate space between the valve and the STJ, allowing for the chimney technique. C) Valve-directed stenting from the coronary ostium towards the valve frame. D) PCI with minimal protrusion, as the coronary ostium is located above the valve. E) Coronary ostium located below the valve frame, with sufficient space between the valve and the STJ to perform the chimney/snorkel technique. F) Coronary ostium located below the valve frame, with limited space between the valve and the STJ; therefore, stenting is directed from the ostium towards the valve. BEV: balloon-expandable valve; PCI: percutaneous coronary intervention; SEV: self-expanding valve; STJ: sinotubular junction; TAVI: transcatheter aortic valve implantation
Final message
TAVI is a popular Aortic Intervention, but the risk of coronary obstruction is often underestimated by cardiologists, and it can happen during the procedure or in the long term; thus, preparedness is essential.
Reference
1.Aquino_bruno.pdf TAVI and coronary interventions: indications, technical considerations, and clinical scenarios Euro Interventions Volume 22 Number 11 Jun 1, 2026



