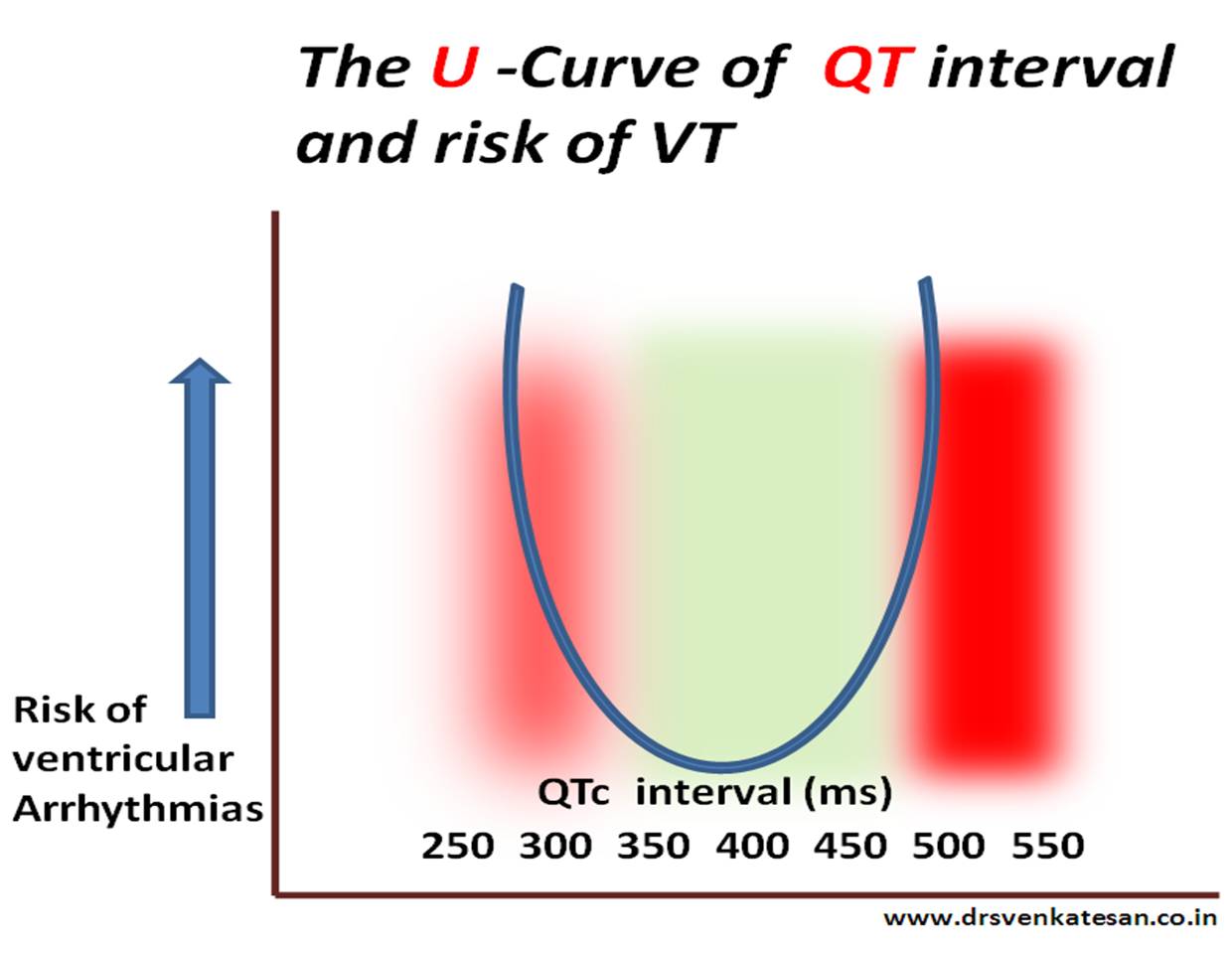
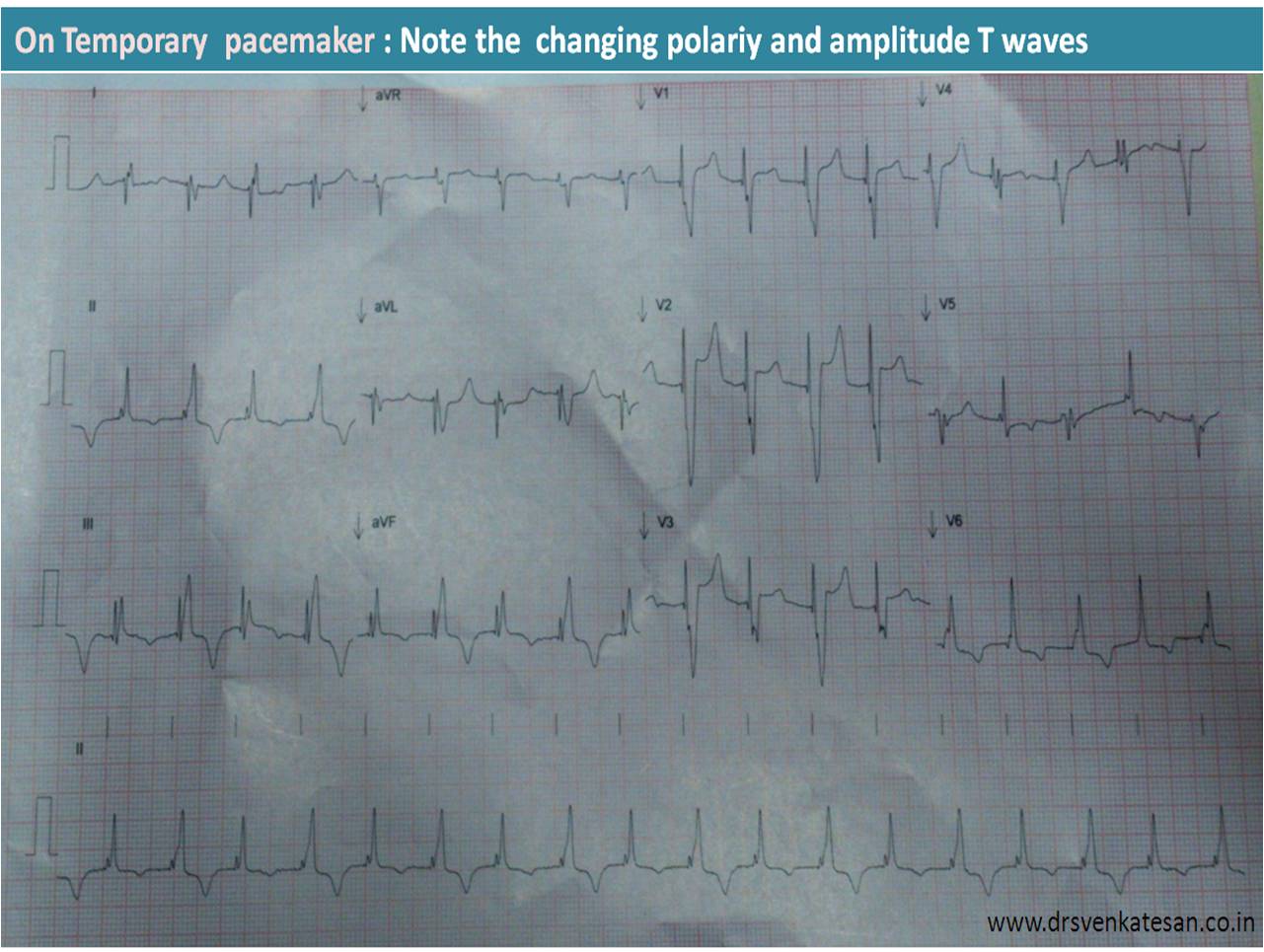
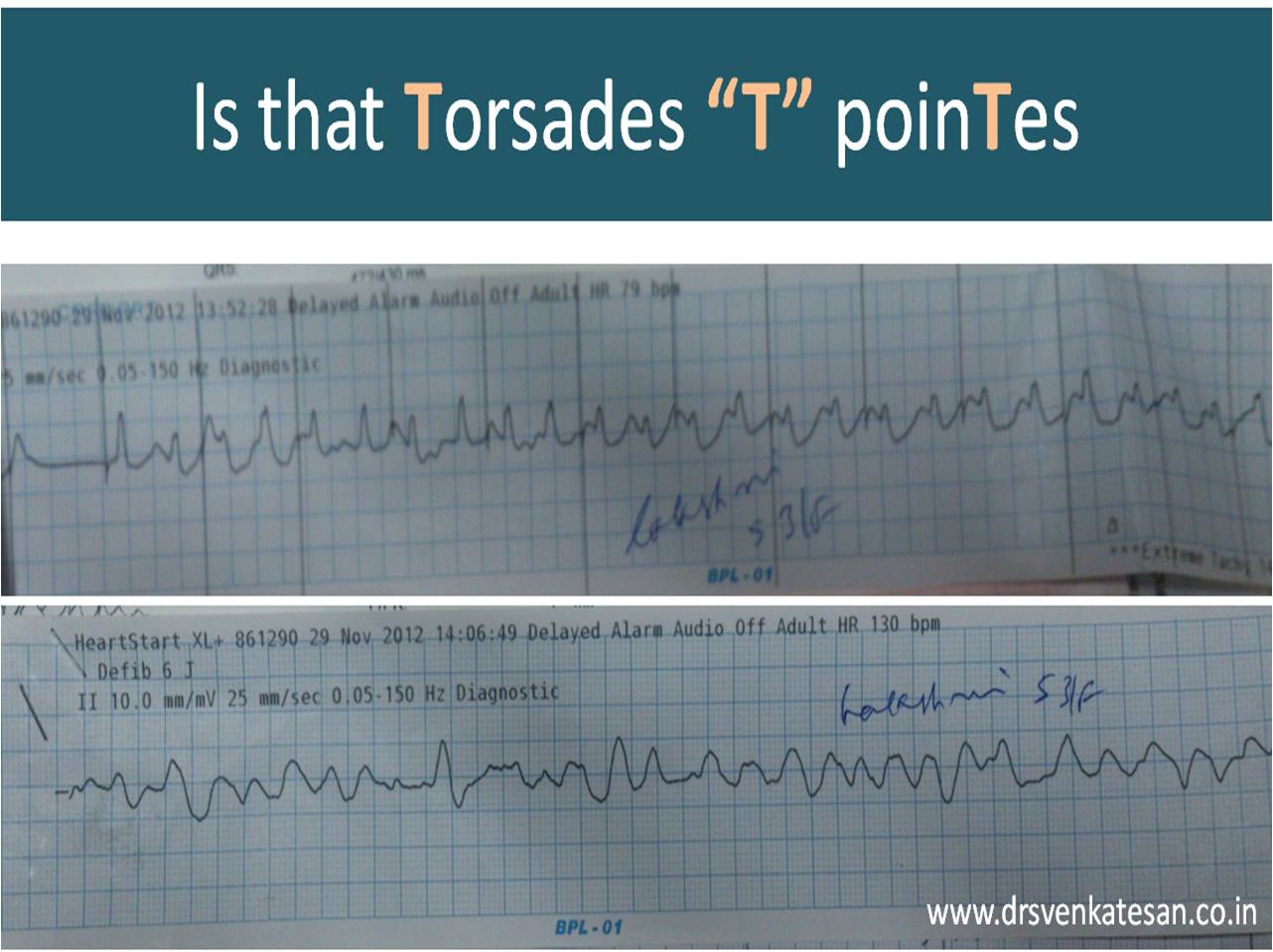
Syncope in CHB is due to unsafe escape rhythm, changing focus of VPDs, extreme bradycardia, (<20 /minute), pause induced VT, (Usually polymorphic and torsades is quite common .) ultimately may end with convulsions, ventricular fibrillation, and death.
Syncope in SND is due to extreme slowing of SA node . Sinus pauses or even arrest can happen resulting in ventricular standstill. Fortunately, a stable escape rhythm ensues more often than in CHB. (It may just be around 20 or 30/mt. still, ventricular arrhythmias are uncommon. ) This implies an important fact that stability is more important than slowness.Fatality is rare in SND.However, the mechanism of syncope in SND is influenced by the integrity of AV conduction also. If it is severely impaired it can trigger ventricular arrhythmias as well as the escape focus becomes unstable infra hisian location.
Paradoxically, in patients with SND, an episode of palpitation due to AF or sinus tachycardia precedes the episode of syncope. An intelligent patient may recognize this as a warning and can take lying posture after runs of palpitation.This is because of tachycardia-induced suppression of SA node prolong the sinus node recovery time still further.
How to differentiate cardiac syncope from simple vasovagal syncope?
Cardiac syncope is differentiated by common vaso-vagal syncope (VVS) as the latter occurs during erect posture . It may be entirely due to vascular component and hence it may simply represent hypotension without a true cardiac limb .(Vasodepressor syncope)
Hence the pulse rate and volume may take some time to recover in VVS, while Stokes Admas of CHB usually have a well-formed bounding pulse in the recovery phase, as the rate is low and systemic hypoxia is a consistent feature.
How is the respiration during Stokes – Adams syndrome ?
Intact. Oxygenation in the lungs goes on for time being. The pooled pulmonary blood gushes after the termination of syncope and causes the classical flushing. Since the hypoxia causes systemic vasodilatation the flushing is more obvious.(Unlike vasovagal syncope where they are often pale)
History of stokes Adam’s syndrome Morgagni is the one who gave credit to their discovery
Though Morgagni first described the clinical picture of this syndrome in 1761, It was published much later by Two Irish Physicians Stokes, Adams. Wish this entity is referred to as Morgagni-Stokes-Adam’s syndrome
Reference
2.W. Stokes. Observations on some cases of permanently slow pulse. Dublin Quarterly Journal of Medical Science, 1846, 2: 73–85