Archive for the ‘Uncategorized’ Category
Peer reviewed perils: Medical science is still far away from true democracy !
Posted in Uncategorized, tagged acc aha esc guidelines, clinical cardiology, drsvenkatesan venkat quotes, medical editors, medical ethics, nstemi, peer reviewed journal, stemi on September 12, 2020|
Technology : Embolic protective device for TAVI,
Posted in tavr tavi, Uncategorized, tagged embolic protective device for tavi tavr, embolx, sentinel. triguard 3 on September 10, 2020|
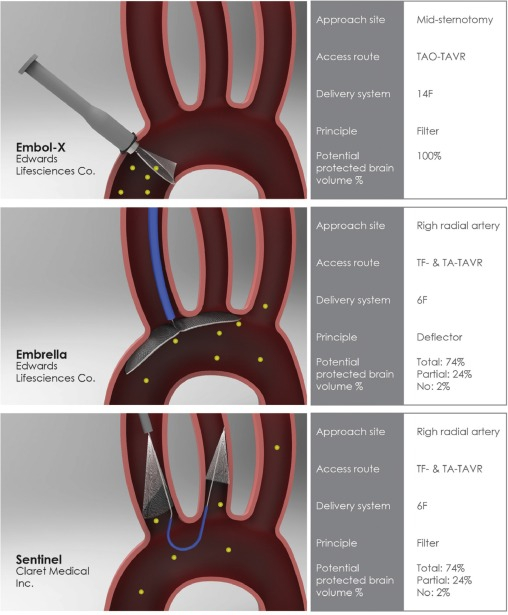
The incidence of stroke during TAVI up to 5 % (minimum ). Stroke risk reduction during TAVI is a critical requirement that can be a deterrent against this wonderful Intervention.
Many devices are being considered
- EmbolX (Edwards life science)
- Emrella
- Sentinel (Claret medical)
- TriGaurd (Keystone)
TriGaurd 3just got the approval from CE and appear promising. (REFLECT trial) It is inserted through the transfemoral route , deflects embolic material to descending aorta since it covers all the three branches of Arch.What happens to these deflected particles? Any bodys guess.
So , in my understanding it converts potential brain embolisation to peripheral microemboli , wh
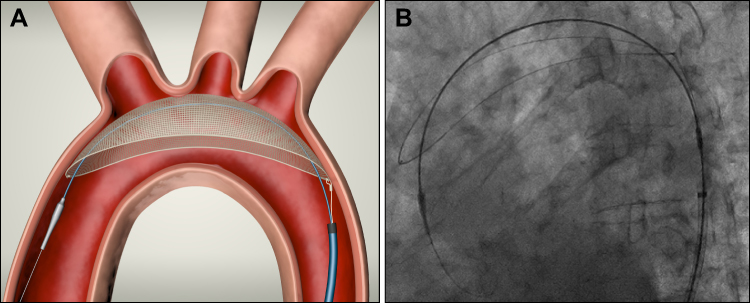
A nice descriptive animation .https://player.vimeo.com/video/232995629
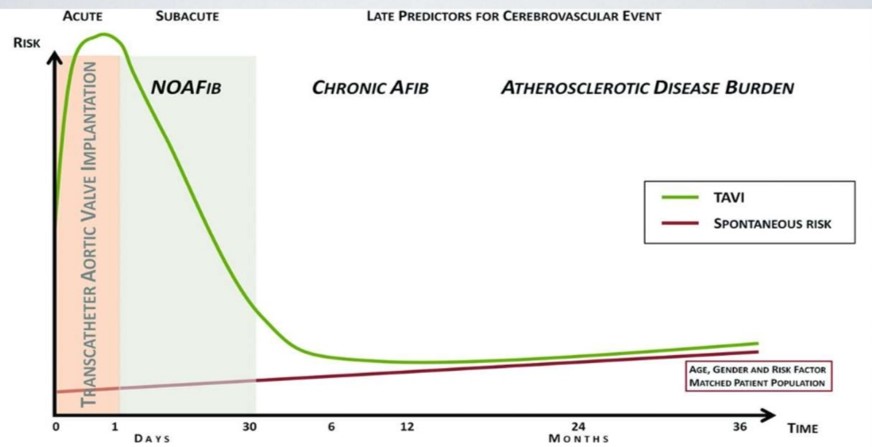
While, these innovative aortic arch filters reduce the risk of periprocedural embolic stroke, please mind, TAVR patients continue to be at significant risk for stroke over a long period. This is due to other late causes like TAVR leaflet thrombosis, atrial fibrillation, arch atheromas, and bleeding due antiplatelet agents.
Reference
Poly-pharmacy : Length of a prescription has a unique story to tell!
Posted in Uncategorized, tagged dr venkat ppt, dr venkat presentations, drvenkatesans, My presentations, polypharamcy, polypill on August 27, 2020|
Can you guess how many drugs a busy physician on an average writes in their prescription in his office ?
Three ? , Five , Six , . . . . Nine,? There is no specific study available for this non-academic query. I have got stunned to see a maximum of 18 drugs in one prescription. So, it should be anything between 1 to 18. May be a mean around 6 or so (Make your own guesstimate)
There is strong evidence to suggest writing a drug prescription has become a (un)conditioned habit-forming act. My professor* used to say generally 2 to 3 drugs are sufficient for most of the common illnesses we encounter (Only in extraordinary situation one may need to go beyond this )
One evidence less estimate though a random observation among the physicians suggested the bottom half of any long list of drug prescription is redundant and it doesn’t really address the specific problem the patient is suffering. Meanwhile ,the concept of poly-pill is making drug compliance easier in many cardiovascular and diabetic diseases.
*William Osler
Final message
Number of drugs human body can handle simultaneously without any harm is often an ignored chapter in the Principles of clinical pharmacology and therapeutics.
Let us mind the length of our prescriptions and ensure less harm to our beloved patients.
Related material
This was my old presentation made about polypharmacy in CHF :Perils and pearls
PDF format of the presentation
PTMC : How to cross a difficult mitral valve ?
Posted in Uncategorized, tagged dr venkatesan ppt, drsvenkatesan ppt, inoue vs accura balloon, mitral valve crossing ptmc, ptmc, retrograde ptmc on August 22, 2020|
Its almost like playing a billiards game in absolute blindness.
It is not an unusual scenerio, to see the balloon catheter delicately bending at IAS puncture site , dodging and deflecting with random jerks as it tries to steal a entry in a few diastolic milliseconds time window when the fish mouthed mitral valve opens in sub square cm areas of MVO trembling in fast atrial fibrillation.
Agree ?
Gathered some tips to cross a difficult mitral valve during PTMC.
This is a PPT presentation taken from archive (Made in 2012)
Please pardon , it lacks audio.
PDF version : Prof SV PTMC mitral valve crossing
Final message
Often times Its noted we tend to struggle more at the mitral valve crossing than at IAS puncture during PTMC. Experience prevails over Image assistance. Assessment of LA size , IAS plane , and sub valvular disease seem to be critical. Probably the secret of success which I found out was , smart guys never hesitate to repeat IAS puncture site for optimal trajectory .Over the wire technique is not forbidden.
Unfortunately, TTE guidance is of little use to cross the mitral valve. Co-registration of fluro/3D TEE is promising , but most cardiologist continue to rely on their experience.
This always Intrigues me ! why we have abandoned retrograde crossing through the Aortic valve that avoids the dreaded IAS puncture. (Refer Dr V.K.Bahl AIIMS Newdelhi in a large series from Greece : Retrograde PTMC J Am Coll Cardiol 1998;32:1009–16)
Most Innovative powerpoint presentation in Echocardiography.
Posted in Uncategorized on August 14, 2020|
I don’t know whether you have seen this before. Surely , I haven’t seen a presentation such as this one.
Place: Annual scientific meet ASE 2013. Minneapolis
Presentor:Dr.Partho Sengupta, Mount Sinai hospital, New york.
Its a 3D presentation in “space” without a screen by Holography.
The stunning 15 minutes lecture take us into the myocardial architecture, with speckles , flow vortex echocardiography and fluid kinetic energy mapping.Don’t miss, a dramatic live teleporting of ASE president on to the stage.
Can you Imagine , where does this technology take us to the future ?
Patients may reach doctor’s offices by holographic teleport for a medical examination or vice versa. Yes, it’s all going to happen someday.
Coronary collaterals in STEMI : Incidence, time of appearance , & Impact on outcome.
Posted in acute coroanry syndrome, acute coronary syndrome, Coronary collateral circulation, Uncategorized, tagged collaterals in stemi, coronary collateral circulation, importance of coronary collaterals in acs nstemi, research ideas in cardiology, research topics in cardiology on August 12, 2020|
Coronary collateral circulation is one of the major determinants of symptoms and outcomes in chronic CAD. But, we generally shrug off the value of coronary collateral circulation in acute coronary syndrome. The fact is, it has a myocardial mitigating effect following sudden total occlusion.
When does it appear? We did a small analysis (PDF version)

We found it is noted in 25% of patients. With reference time of appearance, 6% had it within 12hrs and in few, it was noted as early as 6 hrs. One caveat is, we may not know whether its preexisting collateral due to chronic multivessel CAD. I am sorry to note this study did not address the outcome analysis. We however documented patients with good collaterals had negligible wall motion defect and near-normal function post PCI. Some of you can pursue research in this area.
Potential role of collaterals in ACS
- It limits the infarct size
- Keep the myocardium alive and give us time to intervene
- Can converts a potential Q-MI to non-Q MI
- Possibly prevent primary VT/VF and hence dreaded sudden death in early STEMI
- Prevent early adverse remodeling of the left ventricle.
When these points appeared just my assumptions, Dr. Ali Aldujeli, (Lithuanian University of Health Sciences, Kaunas) in his presentation, at TCT 2020 confirms many of them are Indeed true
Final message
I agree, in the era of instant gratification with primary PCI, relying on coronary collaterals may appear a lesser professional virtue. Still, we may need to respect nature. Many times it bails us out.
Current update 2020
Tribute to my professor Dr M.B Pranesh
Posted in Uncategorized, tagged best neurologist India, coimbatore medical college, doyens of neurology India, Dr M.B.Pranesh neurologist, dr pranesh coimbatore tribute neurologist, history of medicine, tribute to dr m b pranesh on August 2, 2020|
Covid has struck hard and this time it has consumed one of the Doyens of Neurology, from Coimbatore, India –Dr.M.B.Pranesh. Privileged to have him as my professor in Coimbatore medical college, my alma mater, watched him in close quarters during my undergraduate and MD days in the late 1980s.
Still recall, how he empathizes with the patient and their family in distress, practiced medicine in the best scientific manner at the same time with a humane and philosophical touch. I can’t forget, how the little genius standing beside the comatose patients In IMCU and tells so precisely the difference between metabolic vs structural coma without even asking for a CT or MRI scan.(We learned with awe, for the first time, how hyponatremia can cause havoc to the brain) I have seen him so tired in many days and sleeping in the ward chair for a few minutes and comes back fresh for the rounds. He used to say sleep is a luxury in our profession. What a statement to make for our generation next.
His favorite quotes are from William Osler and ask us to read the life history Harvey Cushings. He encouraged us, to learn the history of medicine. He was so emphatic to say “Unless we know how our past physicians toiled with their astuteness and hard work, we will not understand the value of clinical medicine”
One of the pure souls who showed us what is the true meaning of teaching, learning, and caring. Got this small clip, wherein he continues to wish us good.
Let his legacy live forever.
A quiz : What is this list & What are the numbers?
Posted in Uncategorized, tagged drsvenkatesan, madras medical college on July 25, 2020|
Mitra clip magic : Switch off LA “V” waves & Aortic pulse will rejoice Instantly !
Posted in Uncategorized, tagged acute mitral regurgitation, left atrium, mitra clip, v waves in mr on July 12, 2020|
Can a bedside echocardiogram help rule out STEMI in patients with suspicious ECG ?
Posted in Uncategorized, tagged diagnostic criteria for stemi, gls in stemi, role of echocardiography in diagnosis of acs stemi nstemi, wall motion defect in stemi by echo on July 3, 2020|
Can a bedside echocardiogram help rule out STEMI in patients with suspicious ECG?
No, it can’t (Though, it may be tempting to use a rapid echo to look for wall motion defect to rule out ACS )
If your answer is No, probably you don’t need to read any further in this post.
Diagnosis of STEMI* is based on
- Clinical
- ECG
- Bio-Markers
*Please note, two of the most popular investigations namely Echo and Coronary angiogram are missing in the list.
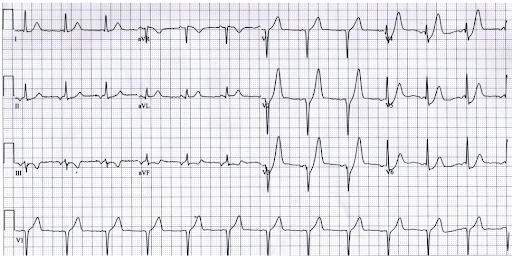
A middle-aged man with chest pain. Can an echocardiogram help you confirm STEMI here? Most likely not. It may still be an evolving STEMI. But, observation, serial ECGs, and Troponin is the answer. (ECG -Source http://www.emdocs.net/hyperacute-t-waves/ )
Though, echocardiography, a great noninvasive imaging tool at the point of care, it stands almost helpless in the diagnosis of the commonest cardiac emergency ie ACS. It can be called as mother of all paradox even visualizing the myocardium directly with high-quality imaging will not tell you, whether there is ongoing ACS or not.
Relying on wall motion defects without diagnostic ECG changes to diagnose STEMI can be misleading for the simple reason, both unstable angina and old MI can be a 100 % confounding effect. Similarly, absence of WMA doesn’t rule out an evolving STEM(Apart from the bizarre behavior of Ischemic cascade, In the early hours only subendocardial wall stress is noted, that is not good enough to cause visible WMA)
Role of CAG in the diagnosis of STEMI
Urgent CAG is an easy way out in confusing coronary conundrums. But, unless you know the background info even a CTO can be mistaken for ATO/ STEMI . So it is essentially new ST/T shifts (corroborated with CAG) will be the guiding force.
Final message
The humble Clinical examination and ECG will prevail over all other modalities in the diagnosis of ACS. Mind you, ECG findings are built within the diagnosis of myocardial infarction ie STEMI (ST-segment) so can’t diagnose it with Echo. Further, an indication of thrombolysis or PCI goes with ECG finding only.
Counterpoint
*Having said that, there is a key role for echocardiography in the ER to diagnose alternate cardiac emergencies like Aortic dissection, Acute pulmonary embolism or ACS mimickers like HOCM, etc. Further, echocardiography is used in a big way, in the risk stratification or identifying complication during the ACS management.
Exceptions
In patients with atypical presentations, pacemaker rhythms, LBBB, especially elderly, comorbid, ECG can be quiet normal or non-diagnostic. Here, echo and angiogram may have some adjunct diagnostic roles.
What about newer echo Imaging modalities?
** There has been a suggestion, that regression of Global longitudinal strain(GLS) or new-onset regional loss of myocardial strain, detected by speckle tracked echo is a powerful and the earliest sign of myocardial ischemia.
A potential tool to rule out ACS by Echo -Global /Regional longitudinal strain (GLS) still trailing behind ECG.
GLS is proposed to be used in coronary units to rule out ACS. In spite of its Initial promise, we understand it has not been accurate enough to be included as criteria to diagnose ACS . So, as of now, it appears unlikely for echo criteria to be included in the diagnose of STEMI.
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- March 2026 (6)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,635,926 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

