Truely a great demonstration of life saving Mitra clip procedure.
Found this from
Posted in Uncategorized, tagged acute mitral regurgitation, left atrium, mitra clip, v waves in mr on July 12, 2020|
Posted in Cardiology - Clinical, cardiology -ECG, Cardiology -unresolved questions, Cardiology hypertension, tagged circulation, diastolic dysfunction, diastolic dysfunction by ecg, doppler e a velocity, e propogation velocity, e vs e', hba1c and left atrium, hypertension, la size in hypertension lae and lvh, la volume, left atrium, limitations of doppler, mitral annular velocity, tissue doppler on May 29, 2011| Leave a Comment »
We presume ECG fails miserably against echocardiography for assessing hemodynamics , while echocardiogram has little value when it comes to studying electrophysiology . Ironically , we often ignore the fact , ECG can provide important long-term hemodynamic data . The pattern of chamber enlargement give us vital clues to the prevailing hemodynamic stress and loading conditions. While echo can be termed as an anatomical and physiologic modality , ECG apart from its unique capacity to record cardiac electrical finger prints , it provides useful , anatomical , hemodynamic information too !
While Doppler is a fascinating modality to measure hemodynamic data in a moment to moment fashion it can never ever tell us , what has been going around in the preceding months or years. This is were chamber size helps which give us chronic physiological information (Chronic Doppler ?)
A simple E:A reversal in mitral inflow doppler can be a innocuous finding in isolation . If it is associated with even minimal grades of LAE it gains huge importance. That is why left atrial size is funnily referred to as HB A1C of diastolic dysfunction ( A marker of chronicity of diastolic dysfunction)
If LAE is so important to diagnose diastolic dysfunction , why we are so obsessed with doppler filling profiles of mitral valve ,pulmonary veins, mitral annular tissue Doppler and what not ! .Many of these sophisticated doppler methods are extremely operator dependent and are subjected to technical and mathematical errors. Especially , with tissue doppler where we magnify the errors as we filter extremely slow tissue motion .
For many decades we have failed to impress ourselves , about the importance of subtle P wave abnormalities in the ECGs of hypertensive patients.
In fact those innocuous looking slurs and notches in P waves , suggest the left atrial stress and a definite marker of underlying LV diastolic dysfunction .
P wave is the only electrical wave that occur in diastole .Hence there is no surprise ,i gives us enormous information about this phase of cardiac cycle .
If only we look at them carefully, zoom it (Now it is made easy with so many softwares) analyse critically we can find a wealth of information about the atrial behavior in hypertension.

Experience from our hypertension clinic with periodic echocardiograms suggest , the following ECG findings can be good markers of significant diastolic dysfunction .
* Surprisingly , these abnormalities correlated with at least grade 1 diastolic dysfunction even in the absence of for LAE or LVH by echocardiogram.
** In an occasional patient P waves can widen due to inter atrial block or conduction delay. This a rare exception for wide P waves without LAE.
Final message
A well recorded and analysed ECG can predict diastolic dysfunction with fair degree of accuracy .This fact need to be emphasized by every one . Next to ECG , LA size and volume by 2d echo are excellent parameters to assess diastolic function in a long term fashion. Sophisticated but error prone , momentary doppler parameters are getting too much attention at the cost of simple , shrewd ECG and 2D echo !
Posted in Cardiology - Clinical, cardiology -congenital heart disease, echocardiography, Uncategorized, tagged echocardiography, left atrium, papvc, pulmonary vein imaging, pulmonary veins, pulmonary venous ostium, pv, right lower pulmonary vein, right upper pulmonary vein, tapvc on March 6, 2010| Leave a Comment »
Even though it is a great vein , often the imaging pulmonary veins by echocardiography is a not a pleasant excercise.
This is due to the following facts
Hence no fixed imaging angle can be advised . But generally a pattern is observed.
Other modalities for imaging pulmonary veins
TEE : Can be very useful since it is brings the vein closer to the probe .But needs more expertice.
Contrast echo :Probably a simple and best modality often underutilised.
Very useful to clinch the diagnosis when PVs take abnormal course as in PAPVC .
MDCT , Spiral CT, MRI are the new age modalities that can provide us with dramatic 3d images of PVs.
The echocardiogram will always prevail over these sophisticated gadgets for its simplicity and also it’s ability to give us the physiology of pulmonary venous flow which is vital in many diseases(Constriction, Diastolic function etc)
The following illustration is a gross attempt to simplify the imaging of PVs.Please note the rules may not be applicable in all.


Left upper and lower pulmonary veins in short axis view will be posted shortly .
Reference
The images are based on personal observations and an excellent insight on the topic from Department of Cardiovascular Medicine, Guangdong Provincial People’s Hospital, Guangzhou , China

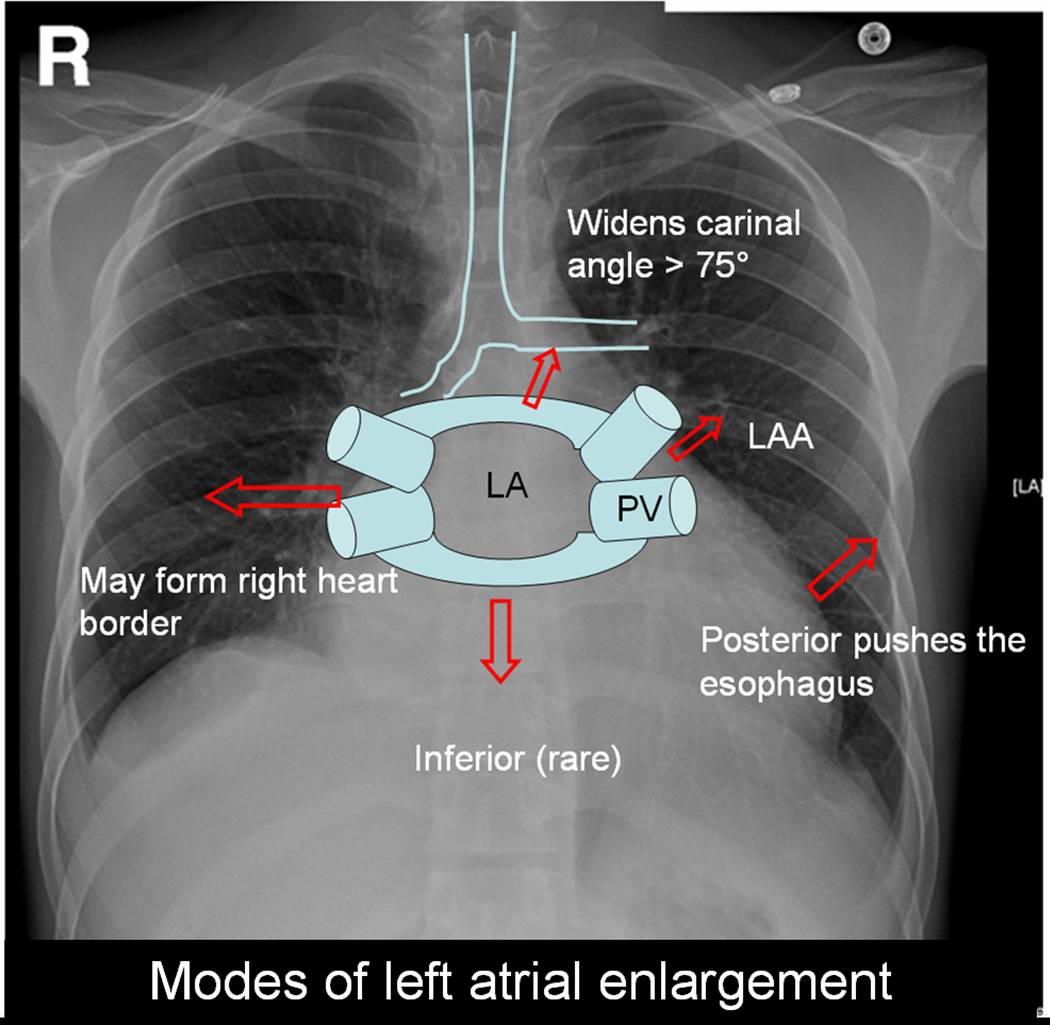
Posted in Cardiology - Clinical, X ray, tagged annals of radiology, atrium, barium swallow, cardiology, carinal angle, chambers of heart, drsvenkatesan, lancet, left atrial volume, left atrium, left heart border, mitral stenosis, nejm, radiograpgy, radiology, rheumatic heart disease, right heart border, X ray on September 18, 2008| 1 Comment »
Left atrium is the posterior most chamber of the heart. It is almost a mid line structure. The normal size of left atrium is about 4 / 4 cm. Normal left atrial volume is 46ml in men and 38 ml in women .(Atrial volume in a normal adult population by two-dimensional echocardiography Y Wang, Chest, Vol 86, 595-601.) Left atrium is not an easy chamber to identify in the X ray chest as it does not form the cardiac border.( Except a small circumference of left atrial appendage.(LAA)
Left atrium can enlarge in multiple directions.Generally it dilates in the path of least resistance.
With the advent of echocardiography X ray assessment of LA is redundant .(Academic value and in fellows training programs).The upper limit of normal LA size is around 4.5cm.
In all these conditions if atrial fibrillation occurs LA size increases further.
Posted in Uncategorized, tagged drsvenkatesan, hypertrophy, left atrium, mitral stenosis, stem cell on July 2, 2008| Leave a Comment »
The left atrium always dilate to pressure overload.And it almost never hypertophies even whne the mean LA pressure raises to high levels. Why ?
1.The atrium basically has little muscle cells to hypertrophy.The left atrial thickness is only 2mm.
They are basically designed to passively fill the ventricles. But this is not always true physiologically.We
call it as booster pump and 30% of LV filling is contributed by active pumping of left atrium.
2. The second reason for left atium not gettting hypertrophied is , there are four decompressing exits
(safety valves) in left atrium namely, pulmonary viens. In fact it’s a paradox the back pressure across
pulmonary circulationmay result in RV hypertrophy
Inference & potential research areas
If by some mechanism if we can induce hypertophy of left atrium will it be a mechanical advantage for left ventricle in failing hearts .By cell therapy we can convert inert atrial cells into activley contracting cells.
DR.S.Venkatesan, madras medical college, Chennai, India .





{kind=link}
{kind=link}